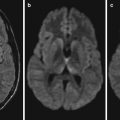
Fig. 14.1
Epidemic encephalitis B. (a, b) MR imaging demonstrates multiple spots of shadows with slightly long T1 and T2 signal in both frontal lobes, basal ganglia, thalamus, and area surrounding posterior horn of the lateral ventricles. (c, d) FLAIR and DWI demonstrate high signal of some lesions (Note: The case and the figures were provided by Gao B from the Radiology Department, Yuhuangding Hospital, Yantai, Shangdong, China)
Case Study 2
A male patient aged 18 years, epidemic encephalitis B.
For case detail and figures, please refer to Handique SK, et al. AJNR Am J Neuroradiol 2006, 27(5):1027.
Case Study 3
A male patient aged 32 years.
For case detail and figures, please refer to Kim SS, et al. Korean J Radiol 2001;2(2):68.
Case Study 4
A patient with epidemic encephalitis B.
For case detail and figures, please refer to Sawlani V. J Neurol Sci 287(1–2):221.
Case Study 5
A patient with epidemic encephalitis B.
For case detail and figures, please refer to Mi YX, et al. Chinese Journal of CT and MRI 2010;8(2):71 (In Chinese).
Case Study 6
A boy patient aged 9 years, epidemic encephalitis B.
For case detail and figures, please refer to Bai GH, et al. Practice of Radiology 2010;25(10):1094 (In Chinese)
14.7.3 SPECT
SPECT of epidemic encephalitis B demonstrates brain lesions at the acute stage with hypertransfusion and, at the subacute and chronic stages, hypoperfusion.
Case Study 7
A female patient aged 58 years.
The lesions of epidemic encephalitis B are located at the central nervous system, which are especially prominent at the cerebral cortex, basal ganglia, thalamus, and midbrain, followed by the lesions at the cerebellum, pons, and medulla oblongata. Autopsy shows diffuse lesions of meningoencephalitis at the gray and white matters of the cerebral hemisphere, basal ganglia, brain stem, cerebellum, and thalamus. Histology reveals brain tissue edema, congestion, capillary hemorrhage, perivascular lymphocytes infiltration, and perivascular brain tissue necrosis. MR imaging demonstrates abnormal signal at the thalamus, midbrain, cerebral cortex, cerebellum, pons, basal ganglia, and even spinal cord. Nearly all cases are demonstrated with lesions at the bilateral thalamus and midbrain, with or without lesions in other brain parts. But there is also a report about case of epidemic encephalitis B with lesions only at the substantia nigra (black matter). The lesions are mostly demonstrated with low or equal T1WI signal and high T2WI signal. Occasionally, hemorrhage is demonstrated at the thalamus and basal ganglia. Contrast MR imaging demonstrates enhancement of the meninges, while usually no abnormal or slight enhancement of lesions at the brain parenchyma. DWI has higher sensitivity to changes in the acute stage than other radiological examinations, although its sensitivity decreases along with prolonged course of the disease. Both T2WI and FLAIR have higher sensitivity in the acute and convalescence stages, especially at the convalescence stage (Fig. 14.2).
Fig. 14.2




Epidemic encephalitis B. (a, b) Transverse FLAIR at day 4 after admission demonstrates patches of high signal at bilateral hippocampus, bilateral thalamus, and bilateral heads of caudate nucleus (indicated by arrow). (c) By follow-up reexamination after 50 days, SPECT demonstrates hypoperfusion at bilateral thalamus and frontal cortex (indicated by arrow). (d, e) Follow-up reexamination after 82 days, FLAIR demonstrates decreased high signal at bilateral hippocampus, bilateral thalamus, and bilateral heads of caudate nucleus (indicated by arrow). (f) Follow-up reexamination after 84 days, FLAIR demonstrates hypoperfusion at bilateral thalamus and frontal cortex (indicated by arrow) (Reprint with permission from Ono et al. (2006))
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
