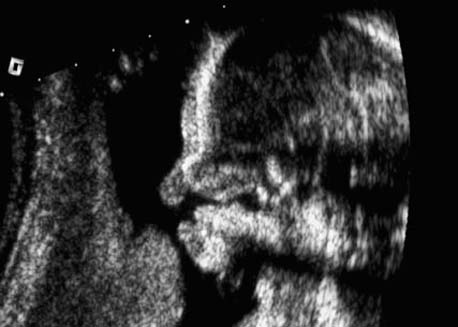
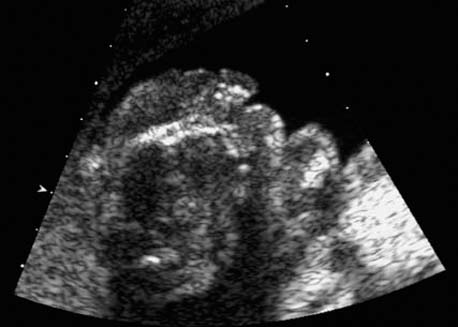
3 Face and Neck Definition: Clefts are defects involving the upper lip and/or the upper jaw and palate; most defects are lateral; they are located medially in less than 1%. Incidence: One in 700–1000 for cleft lip and/or cleft palate and jaw; one in 1000 for cleft palate alone. Sex ratio: M > F. Clinical history/genetics: Mostly sporadic, but may occur often in families due to autosomaldominant, recessive, and X-linked inheritance. If one sibling is affected, the recurrence rate is 4%, with two affected siblings it is 10%. If one parent and one child have this condition, then the rate of recurrence is 14%. Teratogens: Alcohol, maternal phenylketonuria, hyperthermia, hydantoin, aminopterin, methotrexate, metronidazole, carbamazepine, cortisone, radiation, valproic acid. Embryology: Incomplete fusion of the frontonasal process 5–6 weeks after conception. Unilateral or bilateral defects are possible. Associated malformations: If detected prenatally, associated malformations are seen in almost 50%. Over 300 syndromes have been described in association with facial clefts. If the defect lies in the midline, neural tube defects are to be expected, especially holoprosencephaly. Associated syndromes: Van der Woude syndrome seen in 2%, amnion band sequence, arthrogryposis, chromosomal anomalies (especially trisomy 13), holoprosencephaly, Meckel–Gruber syndrome, MURCS association, Nager syndrome, Pierre Robin sequence, Roberts syndrome, short rib–polydactyly syndrome and others. Ultrasound findings: Clefting of the upper lip is seen, and this can be followed up to the palate and the jaw when these are affected. Hydramnios may develop due to an inadequate swallowing reflex. As the fusion of the maxillary bone is completed at 17 weeks, detection of cleft lip may not necessarily mean involvement of the palate and the jaw. Diagnosis of cleft lip can be made as early as 12 weeks of gestation. Clinical management: Screening for other defects and fetal echocardiography. In the presence of other anomalies, karyotyping, parental counseling by an oromaxillary surgeon. Normal antenatal checks, more frequent if hydramnios is present (premature labor). Normal delivery. Fig. 3.1 Cleft lip and palate. Frontal view of the open mouth at 27 + 2 weeks. The continuity of the upper lip is interrupted: one-sided cleft lip. Fig. 3.3 Cleft lip and palate. Same case; small one-sided cleft lip post partum. Procedure after birth: Specific measures are not indicated. Assistance may be required for feeding, depending on individual assessment. Repeated surgical interventions are necessary; correction of the cleft lip is usually carried out during the first 6 months of life. Prognosis: If the finding is isolated, the prognosis is very good; otherwise, it depends on the accompanying anomalies. Midline defects have a poor prognosis, as they are more often associated with other brain anomalies. Self-Help Organizations Title: Prescription Parents, Inc. Description: Support group for families of children with cleft lip and palate. Education for parents of newborns, presentations by professionals. Family social events, phone support network, group development guidelines. Scope: Model Founded: 1973 Address: P.O. Box 920554, Needham, MA 02492, United States Telephone: 781–431–1398 Title: Cleft Palate Foundation Description: Provides information and referrals to individuals with cleft lip and palate or other craniofacial anomalies. Referrals are made to local cleft palate/craniofacial teams for treatment and to parent support groups. Free information on various aspects of clefting for parents and individuals. Scope: National network Founded: 1973 Address: 104 S.Estes Dr., Suite 204, Chapel Hill, NC 27514, United States Telephone: 1–800–24-CLEFT or 919–933–9044 Fax: 919–933–9604 E-mail: cleftline@aol.com Fig. 3.5 Cleft lip and palate. Same case at 22 + 1 weeks; lateral longitudinal view in a case of one-sided cleft lip and palate. Fig. 3.6 Cleft lip and palate. Cross-section of a double-sided facial cleft at 21 + 3 weeks. Outcome: intrauterine fetal death at 36 weeks. Fig. 3.8 Cleft lip and palate. Finding after termination of pregnancy for trisomy 13, confirmed by chorionic villus sampling. Title: Forward Face Description: Mutual support for people with craniofacial disfigurement and their families. Strongly advocates educating members and the public in the quest for understanding and acceptance. Liaison with medical personnel. Newsletter. Videotapes. Teen/young adult support group The Inner Faces. Scope: Model Founded: 1978 Address: 317E. 34th St., New York, NY 10016, United States Telephone: 1–800–393–3223 or 212–684–5 Fax: 212–684–5864 References
Facial Clefts (Cleft Lip and Cleft Palate)






Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


