Fig. 10.1
Hypoechoic nodules . (a) Transverse view of the thyroid demonstrates a nodule (long white arrow) that is hypoechoic or darker than the surrounding thyroid parenchyma (T) but slightly less hypoechoic than the overlying neck musculature (short arrow). This nodule proved to a benign hyperplastic nodule on FNA. (b) Transverse view of the right lobe of the thyroid in a different patient demonstrates a hypoechoic nodule which proved to be a papillary thyroid carcinoma. A lobulated border is noted in this lesion

Fig. 10.2
Hyperechoic nodule . Transverse view of the left lobe of the thyroid shows a nodule (N) which proved to be a follicular variant of papillary carcinoma which is hyperechoic relative to the thyroid parenchyma

Fig. 10.3
Isoechoic nodule . Transverse view of the left lobe of the thyroid shows a solid nodule (arrow) with echogenicity relatively similar to the background parenchyma (T) which proved to be a follicular variant of papillary carcinoma

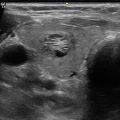
Fig. 10.4
Mixed echogenicity . Transverse view of the right lobe of the thyroid shows a nodule outlined by calipers. The more medial portion of the nodule (straight line arrow) is hypoechoic, and the more lateral portion (dashed arrow) is brighter and isoechoic with the thyroid parenchyma
Most thyroid cancers appear dark or hypoechoic as compared with thyroid parenchyma due to their highly cellular composition. Histologically, the increased cellularity and cellular compaction present in classic papillary thyroid cancer and medullary thyroid cancer produces less acoustic interfaces than micro-follicles and therefore typically causes these lesions to appear hypoechoic compared with surrounding normal thyroid tissue [2, 3] (Fig. 10.1). However, not all neoplasms of the thyroid are hypoechoic in appearance. Follicular neoplasms, including a benign follicular adenoma, a follicular carcinoma, or a follicular variant of papillary cancer, are composed of small micro-follicles with variable amounts of colloid. Therefore, the echogenicity of these follicular-predominant carcinomas and adenomas is less commonly hypoechoic and instead is much more commonly isoechoic or hyperechoic compared with the parenchyma [4, 5] (Figs. 10.2 and 10.3). Additionally, many benign nodules will also appear hypoechoic . Since benign nodules are much more common than malignant nodules, a nodule that is hypoechoic but otherwise lacks any additional features associated with malignancy will statically most likely be benign. Hypoechogenicity , as a unique characteristic of a nodule, is therefore only a moderately sensitive finding for malignancy, with a reported median sensitivity of about 80 %. The reported specificity of hypoechogenecity for malignancy varies greatly depending on the histological subtypes of cancers in the population studied as well as the association of hypoechogenecity with other features and has been reported to range from 36 to 92 % [2, 3, 6–8]. Some authors have identified a sonographic feature called “marked hypoechogenicity ” that describes a nodule with echogenicity that is darker than the surrounding strap muscles [7–9]. Compared to nodules that are hypoechoic with respect to parenchyma but not as hypoechoic as strap muscles, marked hypoechogenicity is less sensitive for identification of thyroid cancer, approximately 41 % sensitive, but much more specific, typically over 90 % [6, 8] (Fig. 10.5).

Fig. 10.5
Markedly hypoechoic nodule . Split screen sagittal (a) and transverse (b) view of a thyroid gland shows a markedly hypoechoic nodule with echogenicity darker than the overlying musculature which proved to be a papillary thyroid cancer. This degree of hypoechogenicity carries a higher specificity for malignancy than hypoechogenicity less than the musculature
The assessment of echogenicity is subjective and tends to have only fair to moderate interobserver reproducibility even among expert observers (Kappa values 0.3–0.5) [7, 10, 11]. Echogenicity can be altered by differing sonographic techniques including changes in the overall gain and transducer frequency. Additionally, in patients with autoimmune thyroid disease such as Hashimoto’s thyroiditis , the echogenicity of the parenchyma is much more heterogeneous in appearance making classification of the nodule’s echogenicity more subjective .
10.1.1 Composition
Nodule composition describes the amount or proportion of solid soft tissue and fluid in a nodule. Nodules can be described as (a) solid, meaning composed entirely or nearly entirely of soft tissue with only a few small scattered cystic spaces (Fig. 10.6); (b) predominantly solid, meaning that soft tissue components comprise at least 50 % or greater of the volume of the nodule (Fig. 10.7); (c) predominantly cystic meaning that soft tissue components comprise less than 50 % of the volume of the nodule (Fig. 10.8); or (d) entirely cystic, meaning fluid filled without appreciable solid component (Fig. 10.9). Some authors have used numerical percentages of cystic or solid elements to describe nodule composition, most commonly by quartiles [1, 12].




Fig. 10.6
Solid composition . Sagittal view of the left lobe shows an entirely solid, hypoechoic nodule which proved to be a follicular adenoma
Fig. 10.7
Predominantly solid composition . (a) Sagittal view of the left lobe shows a predominantly solid, hypoechoic nodule with a few small cystic regions (arrow) which proved to be benign on biopsy. When there are very few cystic regions as in this nodule, some sonologists may classify this nodule as solid. (b) Transverse view of the right lobe of the thyroid shows a predominantly solid, hyperechoic nodule with cystic regions occupying less than 50 % of the volume of the nodule
Fig. 10.8
Predominately cystic composition . Transverse view of the right lobe of the thyroid shows a predominantly cystic, nodule with cystic regions occupying greater than 50 % of the volume of the nodule
Fig. 10.9
Entirely cystic composition . (a) This nodule (outlined by calipers) is completely anechoic without an identifiable solid component. A small echogenic focus (arrow) is related to colloid reverberation artifact. This most likely represents either a colloid cyst or less likely a true cyst of the thyroid and is considered benign. (b) Transverse view of the left lobe of the thyroid in a different patient shows a cystic nodule multiple echogenic foci representing colloid
Thyroid cancers are most commonly solid or nearly entirely solid and are more likely to be solid than benign nodules [1–9] However, because benign nodules outnumber malignant ones, this feature carries a relatively low specificity for malignancy as an isolated feature. It is estimated that a solid nodule has a 15–27 % likelihood of being malignant [12]. Although there is some subjectivity in reporting the degree of cystic change present in a nodule, the interobserver agreement for reporting solid nodule consistency is reported to be quite high [10, 11].
Related posts:
 Ultrasound-Guided Laser Ablation
Ultrasound-Guided Laser Ablation
 Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
 Cytomorphology of Fine Needle Aspiration of Thyroid
Cytomorphology of Fine Needle Aspiration of Thyroid
 The Ultrasound Lexicon: Common Terminology for Thyroid and Parathyroid Sonography
The Ultrasound Lexicon: Common Terminology for Thyroid and Parathyroid Sonography
 Feature Illustration: Vascularity
Feature Illustration: Vascularity
 Pattern Recognition: Diffuse Thyroid Disease
Pattern Recognition: Diffuse Thyroid Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


