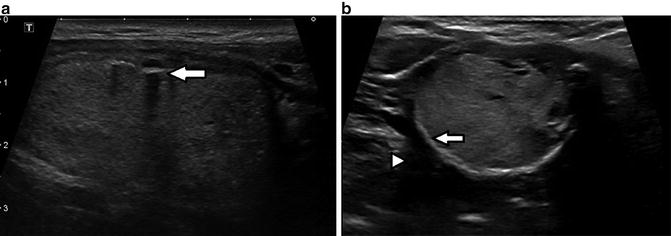
Fig. 12.1
Longitudinal (a) and transverse (b) ultrasound images of the right thyroid lobe. 56-year-old male with a predominately solid-appearing thyroid nodule measuring approximately 2 cm containing punctate echogenic foci with no posterior acoustic artifact (arrows). Biopsy finding was benign colloid nodule (Bethesda II), suggesting that the foci are the back wall of colloid cysts
The significance in trying to differentiate between actual microcalcifications and back walls of cysts or colloid crystals is that the presence of microcalcifications is one of the most specific features of malignancy. Microcalcifications in malignant thyroid nodules are psammoma bodies, which are 10–100-μm round laminar crystalline calcific deposits (see Fig. 12.2). They are found in 29–59 % of all primary thyroid carcinomas , most commonly in the papillary type. The presence of microcalcifications has been noted in follicular and anaplastic thyroid carcinomas as well as in benign conditions such as follicular adenoma and Hashimoto’s thyroiditis. On ultrasound, microcalcifications appear as punctate rounded hyperechoic foci without acoustic shadowing [8–10] [see Fig. 12.3] and may be difficult or impossible to differentiate from benign entities mentioned above such as cyst back walls or colloid. Therefore, an analysis of the presence or absence of the other sonographic features associated with malignancy (such as all solid consistency and infiltrating borders) is helpful in the decision to pursue FNA when this type of echogenic foci is noted.


Fig. 12.2
Micrograph of psammoma bodies (arrows) in papillary thyroid cancer
Fig. 12.3
Ultrasound image of a partially cystic/solid 1 cm thyroid nodule containing punctate foci with no posterior acoustic artifact (arrow) in a 54-year-old female. Biopsy finding was suspicion of papillary carcinoma (Bethesda V), which was confirmed at subsequent surgery
12.3 Echogenic Foci with Small Comet-Tail Artifacts (≤1 mm Long)
A comet-tail artifact is a form of reverberation artifact between two reflective interfaces resulting in closely spaced reflective echoes. The returning sequential echoes may be so close together that individual signals are difficult to perceive, with the later echoes decreasing in amplitude secondary to attenuation. On ultrasound, this is displayed as an artifact with decreased width and signal strength and manifests as a triangular, tapered shape [1, 11, 12] [see Fig. 12.4 and Chap. 5].

Fig. 12.4
Ultrasound image of an irregular margined, predominately solid, and hypoechoic 1.8-cm right thyroid lobe nodule in a 48-year-old female. Echogenic foci with small (<1 mm) comet-tail artifact are present (arrow). Biopsy finding was suspicious of papillary carcinoma (Bethesda V), which was confirmed at subsequent surgery
Traditionally, all echogenic foci with a comet-tail artifact were thought to be a strong sign of benignity. This is because the artifact was thought to be arising from the inspissated crystals of benign colloid nodules [1, 2, 12]. A recent study however has shown that the rate of malignancy of nodules containing echogenic foci with small (<1 mm) comet-tail artifact was similar to those without acoustic artifact (around 15 %) [2]. This finding suggests that some malignant microcalcifications may also demonstrate small comet-tail artifact. This is supported by the literature that shows several forms of calcifications in a variety of organs and of various sizes demonstrate comet-tail artifact [13]. Why some microcalcifications presumably demonstrate small comet-tail artifacts while others do not is unclear but may in part be related to factors such as ultrasound machine settings (e.g., spatial compounding, frame averaging, speckle reduction), transducer frequency, scanning operator variability, and other technical factors. Again, based on these findings, the additional parenchymal characteristics of the nodule need to be closely evaluated in helping to determine if biopsy of the nodule is warranted.
12.4 Echogenic Foci with Large Comet-Tail Artifact (>1 mm)
A recent study demonstrated a very low rate of malignancy (3.9 %) in nodules possessing echogenic foci with large (>1 mm) comet-tail artifact as compared to other echogenic foci. This suggests that these artifacts are most likely secondary to those seen with inspissated colloid crystals in benign colloid nodules . An older study described the comet-tail artifact as a benign feature in avascular cystic nodules likely related to colloid and determined four patterns of the artifact in colloid cysts. In their series, nodules with one of these features showed 100 % sensitivity and specificity for benignity [12]. Thus, a thyroid nodule containing echogenic foci with large comet-tail artifacts in a primarily cystic nodule suggests benignity and may preclude the need for biopsy [2] [see Fig. 12.5].

Fig. 12.5
(a) Ultrasound image of the left thyroid lobe in a 61-year-old woman shows a cystic 2.6-cm nodule containing several echogenic foci with large (>1 mm) posterior comet-tail artifacts (arrow). Biopsy finding was benign colloid nodule (Bethesda II). (b) Schematic representation of the inverted triangle associated with large comet-tail artifact (Image courtesy of Matthew Skalski, medical illustrator, University of Southern California)
12.5 Internal Echogenic Foci with Posterior Acoustic Shadowing
Echogenic foci associated with posterior acoustic shadowing are true thyroid calcifications . In order to cause the shadowing, the calcification is typically larger than 1 mm in size and often much larger and can be quite variable in shape [see Fig. 12.6]. Pathologically they represent fragmented plates, spicules, or granular deposits of calcium within fibrous septa in the thyroid gland parenchyma and/or nodules. In the literature, these foci are commonly referred to as “macro-” or “coarse” calcifications and are thought to be dystrophic calcifications secondary to tissue necrosis. The ACR committee on thyroid ultrasound in their recent publication of a Thyroid Imaging Reporting and Data System (TIRADS) chose the term macrocalcification for this type of echogenic focus [14, 15]. They can be seen in multinodular goiter but also in solitary thyroid nodules. Approximately 15 % of nodules with these calcifications harbor malignancy. Of note, these are the most common type of echogenic foci in medullary type of thyroid cancer [2, 3, 8, 10].

Fig. 12.6
Ultrasound image of a left 2.8-cm solid hyperechoic thyroid nodule in a 59-year-old female. Central shadowing clumped parenchymal calcification is noted (arrow). Biopsy finding was benign colloid nodule with Hurthle cell changes (Bethesda II)
12.6 Peripheral Echogenic Foci with Posterior Acoustic Shadowing
These echogenic foci also are true calcifications and are curvilinear in shape, occurring along the periphery of nodules and are associated with posterior shadowing [see Fig. 12.7a, b]. In the literature, these peripheral calcifications are frequently referred to as “rim” calcifications or “eggshell” calcifications when smooth and regular and extend around the entire nodule. Frequently, the extent of posterior shadowing precludes further evaluation of the internal parenchymal features of the nodule. In fact, in some instances, attempting a biopsy of these nodules is nearly impossible if the periphery is completely circumscribed by calcification. As seen with large internal macrocalcifications, the presence of these foci is associated with an increased risk of malignancy, as compared to nodules without echogenic foci [2]. Nodules that have peripheral calcifications that are irregular in thickness or an interrupted peripheral calcification with soft tissue extending through the rim are highly likely to be malignant [16] [Figs. 12.8 and 12.9].