Fig. 11.1
Visual schematic of margin features applicable to thyroid nodules
It is relevant at this point to clarify an important concept that particularly strikes novice sonographers and trainees in residency and fellowship when first realized and that sometimes escapes appreciation by physicians even with advanced experience. Namely, the distinction between follicular adenomas and follicular carcinomas exists at the level of the nodule margin (Fig. 11.2a, b), not at the level of the thyroid gland capsular margin. Capsular invasion of follicular carcinomas is histologically detected at the margin that surrounds the nodule; vascular and lymphatic invasion can be present at that same margin and also within the nodule [15]. This is in contrast to extrathyroidal extension: in Fig. 11.2c, d, papillary thyroid cancer (PTC) cells are seen nestled beyond the thyroid border but not beyond the pathological inked margin. Figure 11.2e demonstrates these relationships in an ultrasound image.


Fig. 11.2
Surgical total thyroidectomy specimen seen intact (a) and sectioned (b) to reveal a benign follicular adenoma (tan oval) surrounded by reddish normal thyroid parenchyma. It is this interface between the edge of the adenoma and the thyroid that represents the margin visible by ultrasound and also the border at which vascular or capsular invasion would indicate a follicular carcinoma. In contrast, a large papillary thyroid cancer is shown within the left thyroid lobe (c) to have an irregular periphery that extends up the surface of the thyroid gland, leaving no intervening normal thyroid tissue. Microscopic view (d) shows that the papillary thyroid cancer extends outside the thyroid capsule into the perithyroidal fat (white foamy material in top right corner) and up to the histologic margin (the think black inked line visible along the top of tissue). Thus, there are different applications of the term “margin” in relation to nodules and thyroid specimen. (e) Margins of nodules versus pathologic margins of surgical specimens. Yellow dotted lines are size caliper markings of a small thyroid nodule. The blue line circling the nodule indicates the margin that is relevant for the pathologist in distinguishing follicular adenomas from follicular carcinomas. The arrows outline the capsule of the thyroid gland, which serves as the pathologic margin of a routine thyroidectomy specimen. Shown are two ultrasound views (E1) and a surgical specimen view (E2)
In terms of margins, therefore, there are visual (artistic) and linguistic (poetic) challenges of trying to clarify and codify the pathology of thyroid disease as detected by an imaging modality like ultrasound . The figures and videos in this chapter are all ultrasound cine clips to emphasize the point that margins are spatially continuous and that a single, still image cannot represent the entire contour of the nodule.
11.2.1 Completely Smooth and Well-Defined Margins
Thyroid cysts represent the classical version of a margin that is completely smooth. The interface between the liquid composition of the cyst provides stark contrast to the solid thyroid parenchyma, and thus the ultrasound wave physics translate that contrast into a hyperechoic thin line as the border (Fig. 11.3). The terms well-defined and well-circumscribed are likewise interchangeably used. The connotation of these terms is that it is visually clear to see the margin and to appreciate that there is a distinct structure (nodule) embedded within surrounding thyroid parenchyma. The contour of the structure can be readily traced on the ultrasound monitor. Representative images and cine clips of both cystic and solid nodules with smooth margins are shown in Video 11.1a–e.

Fig. 11.3
Example of a cystic nodule in the left lobe adjacent to the common carotid artery that has a smooth cyst wall
11.2.2 Lobulated Margins
This describes the geometric path of the margin, resulting in forms that make the nodule appear to have curved or wavy additional segments. The actual line of the margin can vary in thickness and smoothness and even display infiltrative characteristics. Insufficient data have been reported to know the independent risk of malignancy when a lobulated margin is observed in the presence or absence of other features. Representative surgical images (Fig. 11.4) (medullary thyroid carcinoma ) and cine clips of nodules with lobulated margins are shown in Video 11.2a–e.

Fig. 11.4
Lobulated margins in medullary thyroid carcinoma (a—intact pathological specimen, b—sectioned lobe)
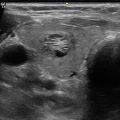
11.2.3 Irregular Margins
The appearance of anything but a smooth border raises the concern for potential malignancy. The assessment that a margin is irregular implies that an actual border can be detected (in contrast to an indistinct border). There are varying manifestations of irregular margins. Some can appear smooth for the majority of the circumference or contour but have an area where the line is jagged; other nodules have a jagged margin at all points. Careful assessment of the entire margin of the nodule is therefore necessary as illustrated in Video 11.3. The majority of the nodule has a well-defined margin, but the inferior aspect is irregular and jagged. In the ATA classification, the presence of an irregular and jagged margin sorts the nodule into a high risk of malignancy category and in TIRADS, at least into category 4 [10, 12–15].
The relationship between echogenicity of the nodule and degree of irregularity of its margins is not fully understood by most experts, mainly due to lack of data, so as to allow clear classification into an ATA or TIRADS category [10, 12–15]. This combination has not been formally assigned to a risk of malignancy pattern or classification. While hyperechogenicity mostly favors a benign nodule, and irregular borders are generally exceptionally rare with benign nodules, the combination of these features has unknown diagnostic associations.
Representative cine clips of a variety of irregular margins are shown in Videos 11.2e and 11.4a–f and Fig. 11.5.

Fig. 11.5
Surgical specimen of nodule (known papillary thyroid cancer) with irregular margins (see also Video 11.4a–f)
11.2.4 Indistinct or Poorly Defined Margins
The pathologic correlation to this feature is related to the invasive nature of malignant cells which gradually encroach into normal surrounding tissues. Because cancers can have a desmoplastic, fibrotic texture which is unevenly distributed along those lines of invasion, the interface with normal thyroid parenchyma can appear blurred. Representative images and cine clips of a variety of these clinical scenarios are shown in Video 11.5a–g. However, since hyperplastic nodules represent a local disruption of the follicular architecture of the thyroid, it is common for these begin nodules to also have a poorly defined margin along a portion of the nodule (Video 11.5f). The typical spongiform appearance of these nodules and the absence of other sonographic features of malignancy, such as all solid consistency and calcifications, help to distinguish these nodules from malignancy .
Related posts:
 Ultrasound-Guided Laser Ablation
Ultrasound-Guided Laser Ablation
 Transcutaneous Laryngeal Ultrasonography: Clinical Variables
Transcutaneous Laryngeal Ultrasonography: Clinical Variables
 Cytomorphology of Fine Needle Aspiration of Thyroid
Cytomorphology of Fine Needle Aspiration of Thyroid
 The Ultrasound Lexicon: Common Terminology for Thyroid and Parathyroid Sonography
The Ultrasound Lexicon: Common Terminology for Thyroid and Parathyroid Sonography
 Feature Illustration: Vascularity
Feature Illustration: Vascularity
 Pattern Recognition: Diffuse Thyroid Disease
Pattern Recognition: Diffuse Thyroid Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


