FIGURE 5.1A
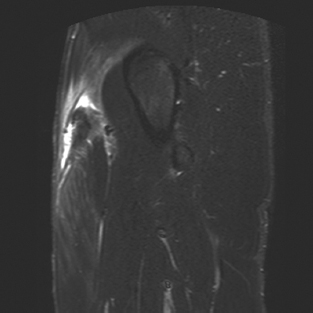
FIGURE 5.1B
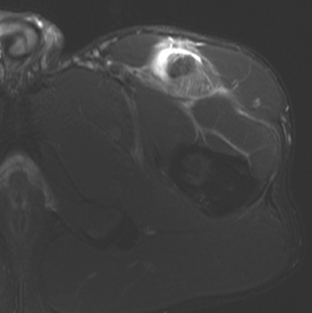
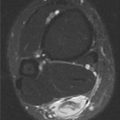
FIGURE 5.1C
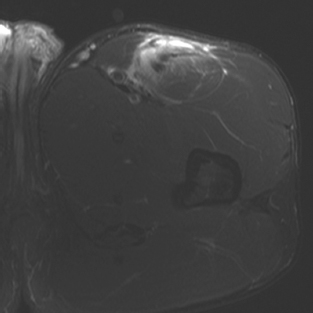
FIGURE 5.1D
FINDINGS
- A, B. Coronal and sagittal T2-weighted MRI with fat suppression show discontinuity and distal retraction of the proximal rectus femoris tendon. The tendon is thickened and redundant, and is surrounded by fluid. Feathery edema is seen along the musculotendinous junction of the rectus femoris muscle belly.
- C. Axial T2-weighted MRI with fat suppression at the level of the femoral neck shows the thickened and retracted rectus femoris tendon, with surrounding fluid and edema.
- D. Axial T2-weighted MRI with fat suppression at the level of the lesser trochanter shows edema along the musculotendinous junction of the rectus femoris.
DIFFERENTIAL DIAGNOSIS none
DIAGNOSIS Rectus femoris strain, grade 3.
DISCUSSION Rectus femoris muscle has two origins; direct or straight head originating from the anterior inferior iliac spine, and the indirect or reflected head originating from the acetabular rim. Avulsion of the direct head is more common than the avulsion of the indirect head because the direct head is taut in the beginning of hip flexion [1]. In this case, both heads are torn from the origin, with inferior retraction of the muscle belly and associated hematoma. Unlike the other quadriceps muscles, the rectus femoris is both a hip flexor and a knee extensor; it is thus more vulnerable to injury under tension.
CASE 5.2 CLINICAL HISTORY
A 60-year-old man who fell during yard work.
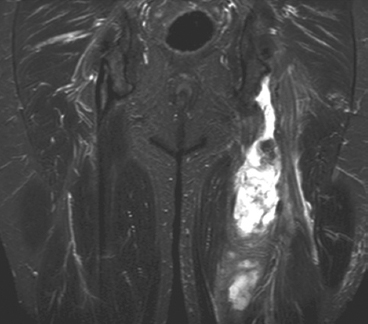
FIGURE 5.2A
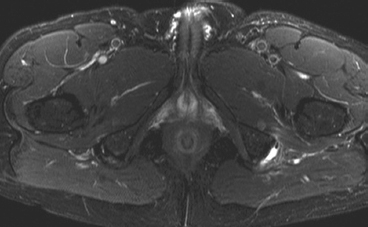
FIGURE 5.2B
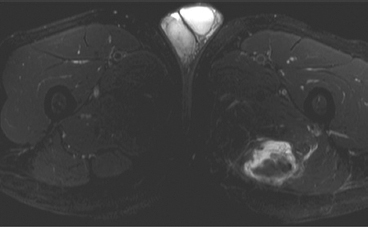
FIGURE 5.2C
FINDINGS
- Coronal fat-saturated T2-weighted MRI image shows a long fluid collection containing debris in left medial thigh, inferior to the ischial tuberosity. Normal right hamstrings tendon is seen.
- Axial STIR image at the level of hamstrings insertion at ischial tuberosities shows normal insertion on right, but no tendons at the left.
- Axial STIR image at midthigh level shows the hematoma and retracted left hamstrings muscle.
DIFFERENTIAL DIAGNOSIS None.
DIAGNOSIS Hamstrings tear with associated hematoma.
DISCUSSION The hamstring muscles, located in the posterior thing, include the long head of biceps femoris, the semimembranosus, and the semitendinosus. They are major knee flexors and also aid in hip extension. Semitendinosus and biceps femoris tendons insert together as a conjoint tendon whereas semimembranosus tendon inserts just lateral to the conjoint tendon on the ischial tuberosity. Various factors can injure the proximal portions of the hamstring muscles affecting the origin of the hamstrings, including the tendinous enthesis, the underlying ischial tuberosity, and the surrounding tissues [2,3]. Chronic attrition can result in insertional tendinosis and/or small partial tears. In young patients, apophysitis can occur from repeated traction injuries. Abrupt injury at the origin from hip hyperflexion and knee extension results in osseous avulsions of the apophysis in children and proximal tendon ruptures in adults.
CASE 5.3 CLINICAL HISTORY
A 62-year-old man with chronic renal failure treated by long-term hemodialysis.
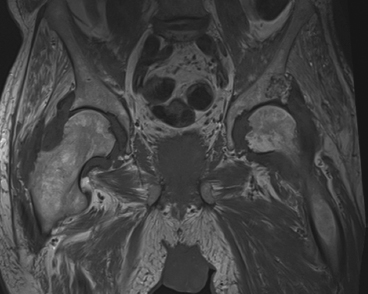
FIGURE 5.3A
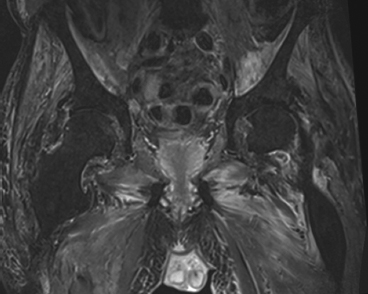
FIGURE 5.3B
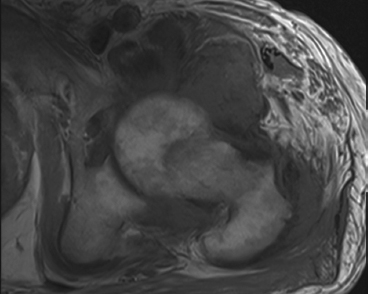
FIGURE 5.3C
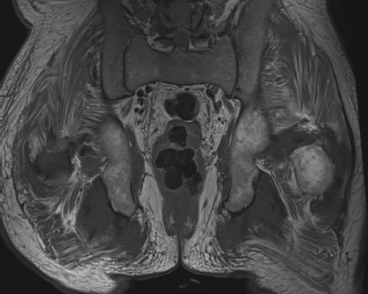
FIGURE 5.3D
FINDINGS
- Coronal T1-weighted MRI through both hips shows intermediate signal masses surrounding both femoral heads and necks. The underlying bones appear intact. Diffuse muscle atrophy is present.
- Coronal T2-weighted fat-suppressed MRI shows that the masses around the hips have low-to-intermediate signal. There is no bone marrow edema.
- Axial T1-weighted MRI of the left hip shows intermediate signal masses around the femoral head and neck, with particular prominence anteriorly. Similar masses involve the tendon insertions at the greater trochanter.
- Coronal T1-weighed MRI through the ischial tuberosities shows masses involving the bilateral hamstring origins.
DIFFERENTIAL DIAGNOSIS Amyloidosis.
DIAGNOSIS Dialysis-related amyloidosis.
DISCUSSION The differential diagnosis revolves around the distribution of abnormalities. The bilateral symmetry makes infection and neoplasm very unlikely. The low-to-intermediate T2 signal of the masses suggests a noninflammatory process, and if gadolinium had been given intravenously (contraindicated in renal failure), one might have seen no enhancement; intense enhancement would be expected in a disease such as rheumatoid arthritis. These features and the involvement of joints and tendons suggest a form of chronic deposition disease. The prevalence of dialysis-related amyloidosis is related to the number of years of hemodialysis and is present in virtually all patients who have had 20 or more years of hemodialysis [4]. The underlying pathophysiology is accumulation of a protein in betapleated sheets or similar configurations. Unlike other forms of amyloidosis, dialysis-related amyloidosis primarily affects the musculoskeletal system and tends to spare the visceral organs until late in the course. Imaging features include periarticular masses of low-to-intermediate signal on T1- and T2-weighted MRI, pressure erosions of adjacent bone, and masses in tendon and muscle [5]. Other common manifestations include destructive spondyloarthropathy and carpal tunnel syndrome.
CASE 5.4 CLINICAL HISTORY
A 54-year-old alcoholic man with worsening bilateral hip pain.

FIGURE 5.4
FINDINGS Anteroposterior (AP) radiograph of both hips. Both femoral heads are sclerotic and show subchondral fractures of the weight-bearing superior quadrants. Step-off at the lateral margins of both articular surfaces indicates the amount of collapse—a few millimeters in this case. There is relatively little acetabular disease.
DIFFERENTIAL DIAGNOSIS Osteonecrosis, osteoarthntis.
DIAGNOSIS Osteonecrosis.
DISCUSSION The principal differential diagnostic consideration is osteoarthritis. The severity of the femoral head involvement with the relative sparing of the acetabulum indicates that the primary process is in the femoral head rather than the hip joint. Secondary osteoarthritis develops soon after femoral head collapse in osteonecrosis, but that is not yet seen in this case. Some patients with osteonecrosis present with the abrupt onset of hip pain, but femoral neck fracture is generally not a consideration without a history of falling or trauma. Most bones have a dual blood supply through the rich network of vessels that supply the periosteum and the ramifications of the nutrient arteries that supply the endosteum. Portions of bone that are covered with articular cartilage, or that are enclosed within joint capsules, have no periosteum and therefore have only an endosteal blood supply, leaving them more vulnerable to ischemic infarction. The femoral head is the most important clinical site of osteonecrosis because of its critical weight-bearing function.
Men are affected by osteonecrosis of the femoral head more often than women by a 4:1 ratio, and the usual age range of patients at presentation is 30 to 70 years. Known causes of osteonecrosis include sickle cell disease, Gaucher disease, corticosteroids, trauma, alcoholism, collagen vascular diseases, renal transplantation, and pancreatitis, but many cases are idiopathic [6]. The typical clinical complaint is abrupt onset of hip pain without trauma. In 50% of cases, bilateral involvement is present; bilateral disease is usually asymmetric. After the ischemic event, the infarcted, avascular region becomes revascularized from the periphery, and creeping substitution of devitalized bone occurs. When repair begins, plain films may show an increase in bony density around the periphery of the infarction. This increased peripheral density may slowly progress centrally as repair proceeds. Sometimes the dead bone is incompletely resorbed, and a sclerotic zone remains indefinitely. Because this repair process involves both resorption and replacement of bone, the mechanical strength may decrease transiently, and subchondral insufficiency fractures may result. Insufficiency fractures of the subchondral bone may be recognized by a crescentic lucent zone that separates the fragment. This late segmental collapse of the femoral head may rapidly lead to deformity and secondary osteoarthrosis of the hip.
CASE 5.5 CLINICAL HISTORY
A 3-year-old girl with limb-length discrepancy and gait disturbance.
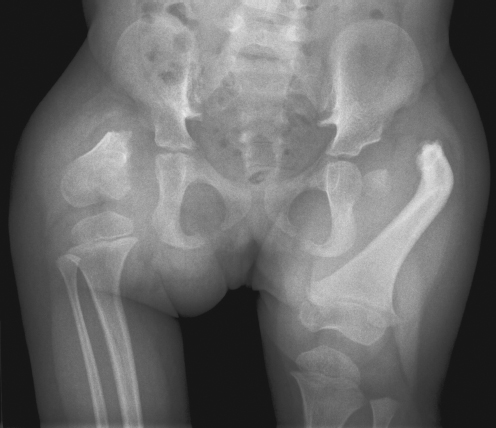
FIGURE 5.5
FINDINGS AP radiograph of the pelvis shows bilateral deficiency of the proximal femurs. On the right side, the femur is very short, with presence of only the distal portion. The acetabulum has not developed. On the left side, a small femoral head is present within a shallow acetabulum. The femoral neck and proximal shaft are absent, and the portion of shaft that is present is dysplastic.
DIFFERENTIAL DIAGNOSIS Developmental dysplasia of the hip, proximal focal femoral deficiency (PFFD), postsurgical state.
DIAGNOSIS Proximal focal femoral deficiency.
DISCUSSION Aplasia, present in this case on the right, is not an aspect of developmental dysplasia of the hip. There is no normal development of the acetabulum or the portions of the femur present, suggesting the abnormality is not postsurgical or otherwise acquired.
PFFD designates a spectrum of developmental deficiencies of the proximal femur, ranging from shortening and varus deformity of the shaft to aplasia of the femoral head, neck, and proximal shaft. Dysplastic changes in the acetabulum correlate with the degree of femoral head deformity or hypoplasia, and they represent the secondary effects of growth in the absence of a normal femoral head and normal weight-bearing stresses. The superior femoral epiphysis is typically mobile within the acetabulum, but in some cases it may be fixed and fused as part of the anomaly [11]. Congenital but not heritable, the cause of PFFD is unknown. The condition is unilateral more frequently than bilateral. When bilateral, it is usually asymmetric.
CASE 5.6 CLINICAL HISTORY
A 38-year-old woman with right hip pain. A, radiograph, B, bone scan, and C, MRI at presentation.

FIGURE5. 6A
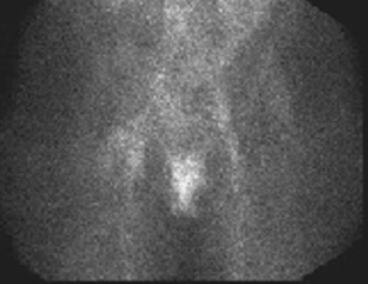
FIGURE5.6B
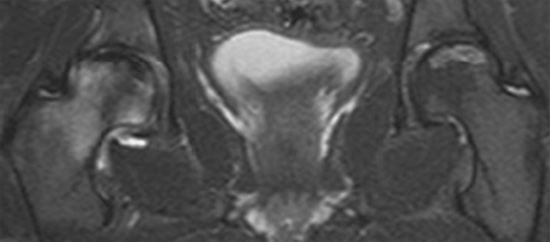
FIGURE5.6C
FINDINGS
- AP view of the right femoral head showing a crescentic subchondral lucency.
- Anterior nuclear medicine blood pool image demonstrateing increased radiotracer uptake at the right hip.
- Coronal T2-weighted fat-suppressed MRI through both hips shows bilateral abnormalities. On the right side, the normally low-signal fatty marrow of the femoral head and neck shows extensive marrow edema. The very low signal crescentic line along the weight-bearing surface corresponds to the subchondral fracture seen on the radiograph. There is a small right hip effusion. On the left side, there is a serpiginous high-signal line along the weight-bearing portion of the femoral head, with normal low signal from the fatty marrow on both sides of the line.
DIFFERENTIAL DIAGNOSIS Osteonecrosis, fracture, septic joint, osteomyelitis, transient osteoporosis.
DIAGNOSIS Osteonecrosis.
DISCUSSION In this case, the left femoral head shows a region of previous osteonecrosis with repair. The right femoral head is acutely osteonecrotic, with extensive marrow edema. Osteonecrosis begins with interruption of the blood supply to the femoral head. The precise event that initiates the loss of circulation may be unknown, although a large number of clinical conditions appear to be associated with it. One possible event is an increase in intraosseous pressure within the femoral head; when this pressure exceeds the perfusion pressure, blood flow stops. Ischemic necrosis of the marrow and bone follows with the onset of pain, but radiographs will be normal. Intramedullary pressure measurements of the proximal femur will be elevated. The typical distribution of infarction is a wedge-shaped region under the weight-bearing surface of the femoral head. The articular cartilage itself remains viable, because its nutrition is derived from the synovial fluid. MRI best demonstrates early osteonecrosis [6]. The region of infarction is evident as a loss of the normal bright marrow signal on T1-weighted images. The radionuclide bone scan may show changes of initial loss of radionuclide accumulation in the avascular stage, with subsequent variable increases in accumulation in the reparative stage. The nuclear scan is less sensitive than MRI and gives poor anatomic detail. The frequent asymmetric bilaterality of osteonecrosis of the femoral head may complicate interpretation of the bone scan.
Initial treatment of osteonecrosis is controversial. The treatment of osteonecrosis of the femoral head focuses on preserving the normal articular surface, typically by core decompression of the neck and head, or placement of a vascularized fibular graft [7]. As one might expect, the earlier the stage at which osteonecrosis is treated, the better the long-term outcome [8].
CASE 5.7 CLINICAL HISTORY
A 44-year-old woman with severe right hip pain. A, radiograph, B, bone scan, and C-D, MRI at presentation; E, MRI after 6 weeks.

FIGURE 5.7A
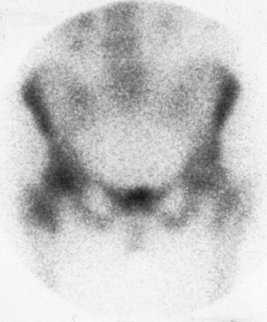
FIGURE 5.7B

FIGURE 5.7C
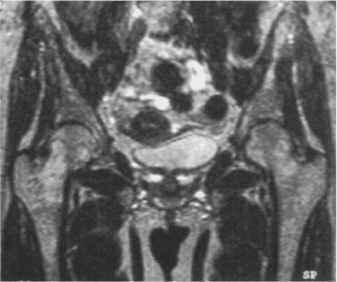
FIGURE 5.7D
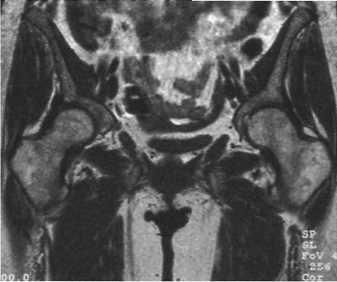
FIGURE 5.7E
FINDINGS
- AP radiograph of the pelvis is normal.
- Bone scan shows increased radiotracer uptake in the right femoral head and neck.
- Coronal T1-weighted MRI of the hips shows loss of the normal bright marrow signal in the right proximal femur, including the entire head and neck.
- Coronal T2-weighted MRI shows edema in the marrow of the entire right proximal femur. There is no effusion in the right hip.
- Coronal T1-weighted MRI taken 6 weeks later demonstrates nearcomplete normalization of marrow signal, indicating resolution of the edema.
DIFFERENTIAL DIAGNOSIS Osteonecrosis, transient bone marrow edema, reflex sympathetic dystrophy, osteomyelitis, fracture.
DIAGNOSIS Transient bone marrow edema.
DISCUSSION In the absence of fracture, the key clinical and radiologic differential diagnosis is between osteonecrosis, which would typically require surgical intervention, and transient bone marrow edema or reflex sympathetic dystrophy, either of which would not. The distinction is clear from the MRI. Transient bone marrow edema is a condition characterized by a rapidly developing bone marrow edema and osteoporosis, affecting periarticular bone that is self-limited, reversible, and has no clear-cut inciting event. It affects previously healthy middle-aged men and women in the third trimester of pregnancy. Its etiology is still unclear, but in view of similarities to regional migratory osteoporosis and reflex sympathetic dystrophy, vascular and neurologic disturbances have been proposed as the possible pathogenetic mechanisms.
Pain in the hip area and functional disability of the affected limb are the main clinical signs. Diagnosis is supported by local radiologic osteopenia whose gradual disappearance parallels the spontaneous recovery. Transient bone marrow edema usually presents with monoarticular joint pain [9]. It typically involves either hip in men or the left hip in women. Self-limited but aggravated by activity, the pain regresses in 2 to 6 months without permanent sequelae. Radiographs are often normal, but they may show a rapidly developing periarticular osteoporosis, particularly in the femoral head, which returns to normal after resolution of symptoms. MRI shows diffuse edema and hip effusion, but no infarction [10]. Bone scans demonstrate increased activity consistent with the bone marrow edema. The initial site of involvement in regional migratory osteoporosis may be the hip, in which case the initial presentation may have been called transient bone marrow edema (osteoporosis) of the hip.
CASE 5.8 CLINICAL HISTORY
A 14-year-old girl with gait problems.
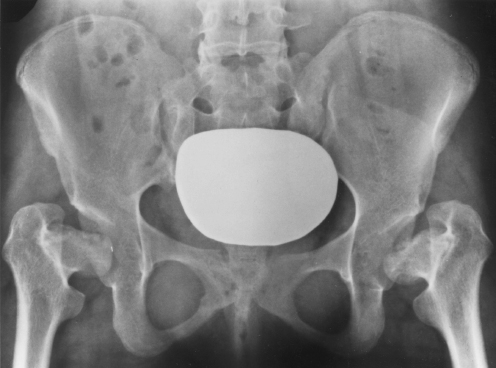
FIGURE 5.8
FINDINGS AP radiograph of the pelvis shows bilaterally small femoral heads with a flattened morphology. Both hips are normally located, but the acetabula are shallow, steep, and dysplastic, to accommodate the abnormal shape of the femoral heads. The femoral necks assume a horizontal orientation but do not appear particularly abnormal in size or shape, given the deformity of the heads. The bones otherwise appear relatively normal.
DIFFERENTIAL DIAGNOSIS Multiple epiphyseal dysplasia, spondyloepiphyseal dysplasia, Legg- Calvé-Perthes disease, developmental dysplasia of the hip, slipped capital femoral epiphysis (SCFE), achondroplasia, juvenile chronic arthritis, mucopolysaccharidosis.
DIAGNOSIS Multiple epiphyseal dysplasia (dysplasia epiphysealis multiplex).
DISCUSSION Bilateral hip disease during childhood may encompass all of the entities in the differential diagnosis. Legg- Calvé-Perthes disease is associated with dysplastic enlargement and flattening of the femoral heads, and juvenile chronic arthritis is associated with epiphyseal overgrowth, cartilage loss, and ankylosis. The hips are normally located, eliminating developmental dysplasia of the hip from further consideration, and although the patient’s age would be typical for SCFE, the radiologic appearance is not. Skeletal changes in the mucopolysaccharidoses may include irregular epiphyses, but biochemical abnormalities will be present clinically, and there is frequent involvement of the thorax and skull, sites that are not affected in multiple epiphyseal dysplasia. The femoral heads in achondroplasia are typically small and dysplastic, with short and disproportionately broad necks, but the absence of bony abnormalities in the pelvis and lumbar spine excludes achondroplasia as a diagnosis in this case. Multiple epiphyseal dysplasia and spondyloepiphyseal dysplasia may be indistinguishable radiographically, except for the absence or presence of spinal column dysplasia. Radiographs of the spine are not included for this case because they were normal.
Multiple epiphyseal dysplasia is a term used to designate a heterogeneous group of disorders that appear to have an abnormality of the epiphyseal chondrocyte in common [12]. Chondrocytes in the growth plates appear to be defective in morphology and organization and deficient in number, with abnormal production of matrix, leading to delayed and disorderly growth and ossification of the ends of the bones. When the hips are involved, the profound loss of growth of the femoral heads results in a markedly decreased range of motion and a waddling gait.
CASE 5.9 CLINICAL HISTORY
A 21-year-old man with limb deformity.
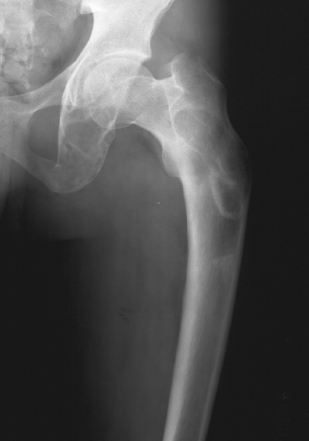
FIGURE 5.9A

FIGURE 5.9B
FINDINGS
- AP radiograph of the left hip. There are expansile lesions in the ischium. There are dysplastic changes in the left proximal femur, with mild expansion and mineralization. The mineralization has a ground-glass appearance; some portions are curvilinear and densely sclerotic. There is a bowing deformity of the proximal femur.
- Follow-up AP radiograph of the left hip after treatment shows osteotomy of the proximal femoral shaft, with intramedullary rod fixation. The bowing deformity has been corrected.
DIFFERENTIAL DIAGNOSIS Fibrous dysplasia, Paget disease, osteogenesis imperfecta, osteomalacia.
DIAGNOSIS Fibrous dysplasia (with shepherd’s crook deformity).
DISCUSSION Bowing deformities of the proximal femur in adults include the items in the differential diagnosis. Paget disease can be eliminated because of the young age of the patient, and the lack of cortical thickening and bony enlargement. Osteogenesis imperfecta would affect all bones and would include osteoporosis as a feature. Osteomalacia, particularly in the setting of renal osteodystrophy, could result in bowing deformity, but other radiologic features should be present. Fibrous dysplasia, both monostotic and polyostotic, commonly involves the proximal femur, and the distinctive shepherd’s crook bowing deformity of fibrous dysplasia is illustrated by this case.
Fibrous dysplasia is a benign fibro-osseous lesion that is neither familial nor hereditary, but appears to be a developmental abnormality involving the proliferation and maturation of fibroblasts [13]. Bowing deformities result from biomechanically insufficient bone, and from malunion of pathologic fractures. Orthopedic management is typically restricted to treatment of complications. The results of curet-tage, bone grafting, and mechanical realignment of proximal femoral lesions are much better in monostotic forms of the disease [14]. Long-term follow-up has shown that bone graft is resorbed and remodeled in fibrous dysplasia.
Malignant transformation has been documented, but it is rare and, in some cases, may have occurred due to previous radiation treatment. Its occurrence has been documented in both polyostotic and monostotic varieties of fibrous dysplasia [15]. These reported secondary sarcomas have been mostly osteosarcomas, but fibrosarcoma, chondrosarcoma, and giant cell sarcoma has also been reported.
CASE 5.10 CLINICAL HISTORY
A young boy with hip problems.
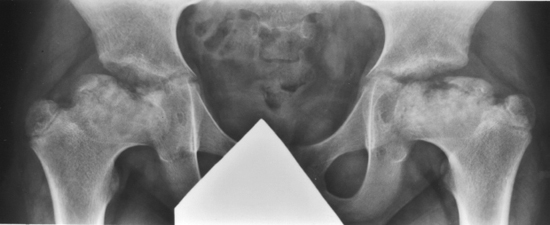
FIGURE 5.10
FINDINGS AP radiograph of both hips shows large femoral heads with short broad necks (coxa magna). The femoral heads are too large to fit fully into the acetabula. The capital femoral epiphyses are enlarged and ossifying from multiple centers.
DIFFERENTIAL DIAGNOSIS Developmental dysplasia of the hip, epiphyseal dysplasia, Legg-Calvé-Perthes disease, SCFE, juvenile idiopathic arthritis.
DIAGNOSIS Legg-Calvé-Perthes disease.
DISCUSSION The abnormalities are bilateral and nearly symmetric, and characterized by enlarged, deformed femoral heads. The relatively mild changes in the acetabula suggest the disease is primarily in the femoral heads. Overgrowth of the femoral heads may occur in juvenile idiopathic arthritis, but there is no apparent joint disease seen in this case. Developmental dysplasia of the hip usually presents in infancy, whereas SCFE usually presents in adolescence.
Legg-Calvé-Perthes disease is idiopathic osteonecrosis of the capital femoral epiphysis in a skeletally immature child. Boys are affected more often than girls by a 4:1 ratio. The mean age of onset is 7 years, and the range is 2 to 13 years.
In 20% of cases, the condition is bilateral. The bone age of affected children is usually 1 to 3 years behind their chronologic age. Interruption of the blood supply to the femoral head leads to partial or total osteonecrosis. Enchondral ossification of the capital femoral epiphysis and activity at the growth plate both stop. The articular cartilage, nourished by synovial fluid, continues to grow. If the disease is detected at this stage, the ossific nucleus of the capital femoral epiphysis will be smaller than normal, and overgrowth of the articular cartilage will be apparent as joint space widening. The patient may be asymptomatic.
Revascularization of the femoral head leads to centripetal ossification, usually from multiple sites that are not contiguous with the original ossific nucleus, resulting in an appearance often described as fragmentation of ossification. Apposition of new bone to the dead bone may increase the radiographic density of the head. Resorption of subchondral bone may lead to subchondral fracture and the onset of clinical symptoms: hip pain and limp. The severity of the clinical findings is highly variable and does not necessarily correlate with the radio-graphic findings. The end result is a short, thick femoral neck and an enlarged femoral head (coxa magna). Premature closure of the growth plate accentuates the deformity. Secondary osteoarthritis is a complication in early adult life.
CASE 5.11 CLINICAL HISTORY
A 65-year-old man with newly diagnosed prostate cancer.

FIGURE 5.11A

FIGURE 5.11B

FIGURE 5.11C
FINDINGS
- A, B. AP radiographs of the hips show multiple oval sclerotic foci present in the femoral head, neck, and intertrochanteric region. A few are noted in the acetabulum.
- C. Axial computed tomography (CT) (bone windows) obtained after intravenous contrast enhancement. There are multiple focal bone densities in the acetabula and proximal femurs on both sides.
DIFFERENTIAL DIAGNOSIS Osteopoikilosis, metastatic disease.
DIAGNOSIS Osteopoikilosis.
DISCUSSION Multiple sclerotic lesions may be seen with metastatic disease, mastocytosis, and occasionally lymphoma.
However, the symmetric periarticular distribution of the sclerotic lesions, their well-defined borders, their uniform size, their oval shape, and their orientation to the long axis of the bone supports the diagnosis of osteopoikilosis. Osteopoikilosis (spotted bones, osteopathia condensans disseminata) is an uncommon osteosclerotic dysplasia with sporadic and familial occurrence. The lesions may increase or decrease in size or number. Symptoms are generally absent or mild, and its discovery is frequently incidental. Histologically identical to bone islands, the lesions have no clinical significance beyond their confusion with osseous metastatic disease [16]. Osteopoikilosis can show increased activity on bone scan [17].
CASE 5.12 CLINICAL HISTORY
A 15-year-old boy with right hip pain.

FIGURE 5.12A

FIGURE 5.12B
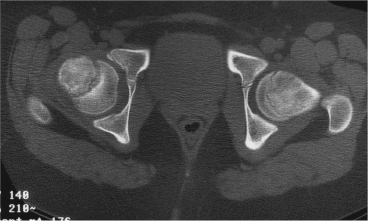
FIGURE 5.12C
FINDINGS
- AP pelvis radiograph shows abnormal right proximal femur. The growth plate appears widened, with irregularity of the metaphyseal margin. The femoral neck appears slightly displaced laterally compared with the capital femoral epiphysis, and an imaginary line drawn along the superior cortex of the femoral neck would not intersect the femoral head (as it would on the normal left side).
- Frog lateral radiograph better shows the abnormal displacement and angulation of the femoral neck relative to the femoral head. An imaginary line drawn along the anterior cortex of the neck would completely miss the head, rather than intersect its margin.
- Axial CT shows the widened, abnormal growth plate and abnormal alignment of neck and shaft. The growth plate has a rounded contour.
DIFFERENTIAL DIAGNOSIS Slipped capital femoral epiphysis (SCFE), healing Salter type I fracture.
DIAGNOSIS Slipped capital femoral epiphysis.
DISCUSSION SCFE is displacement of the femoral head relative to the femoral neck through the open growth plate in an adolescent. The head remains in the acetabulum as the neck progressively displaces anteriorly and superiorly (the head goes inferiorly and posteriorly). SCFE occurs in boys and girls of approximately the same skeletal age shortly before closure of the growth plate (chronologic age of about 11 years in girls and 14 years in boys). Boys are affected more often than girls by a ratio of 2.5:1. Many patients are overweight and have mildly delayed skeletal ages. Bilateral involvement is present in about half of the patients, and some cases are familial. The etiology is not known; the pathophysiology may be related to an endocrine process or a biomechanical problem.
The slippage between the femoral head and neck occurs between the proliferative and hypertrophic zones of the growth cartilage, and early abnormalities of the growth plate may be seen on MRI before changes on radiographs [18]. SCFE is different from a Salter type I fracture, which occurs between the hypertrophic and provisional calcification zones of the cartilage. SCFE may be a chronic, slow process that allows bony remodeling of both head and neck as the deformity progresses, or it may be a relatively acute process (usually lasting less than 3 weeks) whose presentation is not unlike that of a stress fracture. SCFE is treated by stabilization of the head without attempt at anatomic reduction. Pins may be used to fix the position of the head and promote closure of the growth plate. Dysplasia of the hip and early osteoarthritis may develop, and osteonecrosis is a devastating complication that is more common in acute slips.
CASE 5.13 CLINICAL HISTORY
A 5-year-old boy with hip pain and limp.

FIGURE 5.13A
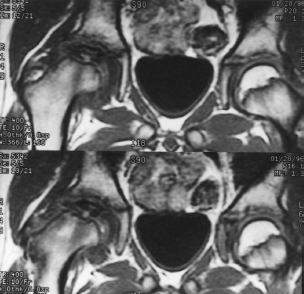
FIGURE 5.13B
FINDINGS
- AP radiograph of both hips. The right femoral head is sclerotic and diminutive. Periarticular osteoporosis is present.
- Tl-weighted coronal MRI shows a low-signal-intensity, small, flattened head. Associated marrow edema (dark on Tl-weighted MRI) extends into the femoral neck. The opposite hip is normal.
DIFFERENTIAL DIAGNOSIS Legg-Calvé-Perthes disease, other cause of femoral head osteonecrosis.
DIAGNOSIS Legg-Calvé-Perthes disease.
DISCUSSION The therapy goal for Legg-Calvé-Perthes disease is to prevent the development of femoral head deformity and subsequent osteoarthritis. Centering of the femoral head within the acetabulum during the revascularization and ossification stages of healing presumably allows the acetabulum to act as a mold for the healing femoral head, averting the development of deformity. Acetabular coverage for the femoral head may be obtained by abduction of the femoral head relative to the acetabulum with a brace, varus osteotomy of the proximal femur, or osteotomy of the pelvis. MRI of the hip may be helpful for estimating the extent of epiphyseal necrosis and delineating the morphology of the uncovered, unossified portion of the femoral head for treatment planning [19,20]. The amount of ultimate deformity depends on the age at onset and the remaining growth potential of the femur. The degree of synovitis accompanying Legg-Calvé-Perthes disease appears to correlate with the extent of epiphy-seal necrosis and the clinical outcome [21]. Osteonecrosis of the femoral head and other growing epiphyses may occur as a result of trauma, infection, sickle cell disease, or other conditions. The pathophysiology and the gamut of radiologic findings are similar to that of Legg-Calvé-Perthes disease.
CASE 5.14 CLINICAL HISTORY
A 45-year-old woman with muscle weakness.
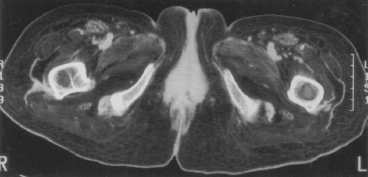
FIGURE 5.14A
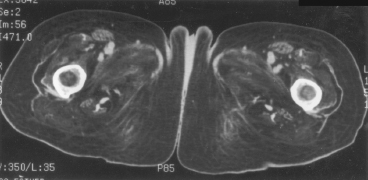
FIGURE5.14B
FINDINGS
- A, B. Axial CT through the proximal thigh demonstrates marked fatty replacement of all the visualized musculature. The bones are normal, with hematopoietic marrow in the proximal femurs.
DIFFERENTIAL DIAGNOSIS Polymyositis, paralysis, corticosteroid excess, arthrogryposis, muscular dystrophy.
DIAGNOSIS Polymyositis.
DISCUSSION Fatty replacement of the musculature may occur on a neuropathic basis or a myopathic basis. In this particular case, the diagnosis is polymyositis and there are no specific distinguishing features. There is a lack of the dysplastic bone and joint changes common in arthrogryposis and muscular dystrophy, suggesting a disease process acquired in adulthood. The presence of soft tissue calcification would strongly implicate dermatomyositis or polymyositis, but none is present on these images.
Clinically, patients with polymyositis demonstrate proximal muscle weakness and pain, which may be progressive or self-limited. This entity may occur with a skin rash (dermatomyositis), Raynaud’s phenomenon, other connective tissue diseases (overlap syndromes), and cancers. The latter association is noted more often in elderly men; however, in general, polymyositis is encountered more frequently in women.
Polymyositis is marked by muscle inflammation followed by atrophy and fibrosis. Soft tissue calcifications may occur in the subcutaneous and deep tissues and, when present, may help distinguish this entity from other causes of muscle atrophy. There is progressive atrophy with fatty replacement, as seen here, which may be demonstrated on CT or MRI [22,23]. The soft tissue changes are best assessed with MRI, which shows increased signal intensity on T2-weighted images within the muscle in the acute setting, and fatty replacement in the chronic setting. Although bony changes are not a feature, arthralgias, contractures, andjuxta-articular osteoporosis may develop. When bony findings such as erosive changes occur, an overlap syndrome or other connective tissue disorders should be considered. Although the primary target of this entity is skeletal muscle, pulmonary fibrosis, pericarditis, dysphasia, and dysphagia may also be present.
CASE 5.15 CLINICAL HISTORY
Acute hip distress in an infant girl with fever. A, radiograph, and B-C, MRI at presentation; D, radiograph after 6 months.

FIGURE 5.15A
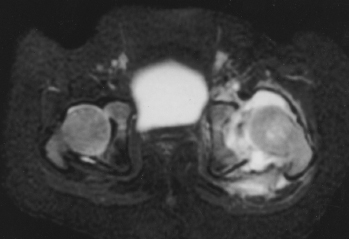
FIGURE 5.15B
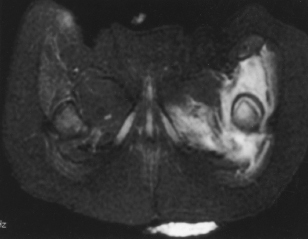
FIGURE 5.15C
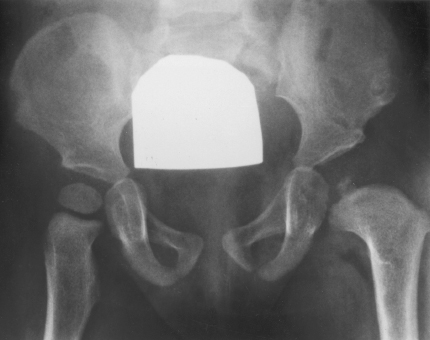
FIGURE 5.15D
FINDINGS
- A. AP radiographs of the pelvis and femurs show lateral subluxation of left hip and periosteal reaction in the femur.
- B, C. Axial T2-weighted MRI demonstrates marked high-signal fluid in the left hip joint, mixed with low-signal debris. This is causing a secondary lateral subluxation of the left hip. Edema is seen in the musculature and soft tissues surrounding the hip.
- D. AP radiograph taken 6 months later shows delayed ossification of the capital femoral epiphysis, with associated underdeveloped concavity of the acetabulum and broadening of the femoral neck.
DIFFERENTIAL DIAGNOSIS Septic arthritis, developmental dysplasia of the hip, Legg-Calvé-Perthes disease.
DIAGNOSIS Septic arthritis, with secondary osteonecrosis of the capital femoral epiphysis.
DISCUSSION The historical facts in this case make the etiology clear. Lateral subluxation of the hip can be the result of mild developmental dysplasia of the hip, but the clinical presentation and the periosteal reaction along the proximal femur is indicative of infection. In the follow-up radiograph, the left proximal femur shows the characteristic changes of osteonecrosis of the growing capital femoral epiphysis: delayed ossification (to be followed by ossification from multiple separate centers), dysplastic enlargement, and a short, broad neck. Sometimes distinction of this entity from Legg-Calvé-Perthes or juvenile idiopathic arthritis can be difficult, and additional imaging should be directed by each child’s clinical presentation [24,25].
Septic arthritis in young children can result from seeding of the joint through hematogenous spread from a remote source, contiguous spread from osteomyelitis, or direct introduction by penetrating trauma. The knee and hip are the most commonly affected sites, and Staphylococcus aureus is the most common organism. The most common presenting sign is that of joint effusion. On sonography, the surrounding capsular structures can be edematous. Juxta-articular osteoporosis quickly ensues due to the aggressive hyperemia. The elicited pannus quickly erodes the cartilage and then bone, leading to joint space loss and associated erosions.
Complications of septic arthritis can include fibrous or osseous ankylosis, synovial cysts, cellulitis or abscesses of the surrounding tissues, osteomyelitis, avascular necrosis, and secondary degenerative joint disease. In this case, the avascular necrosis was presumably a result of an increase in capsular pressure combined with the septic capillary thrombosis.
CASE 5.16 CLINICAL HISTORY
A 75-year-old man with left hip pain after a fall.

FIGURE 5.16A
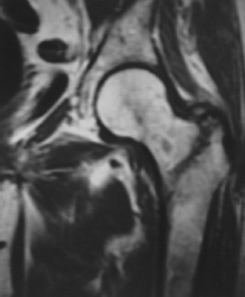
FIGURE 5.16B
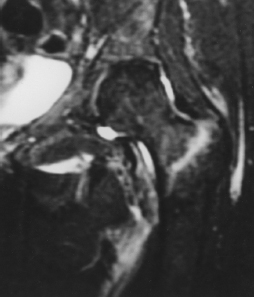
FIGURE 5.16C
FINDINGS
- AP radiograph of the left hip is well positioned (the hip is not externally rotated). The presence of a faint zone of sclerosis in the intertrochanteric region is equivocal and was not prospectively identified as a fracture.
- Coronal Tl -weighted MRI shows a line of hypointensity extending in the sagittal plane between the greater and lesser trochanters.
- Coronal T2-weighted, fat-suppressed MRI shows a line of hyperintensity in the intertrochanteric region, thicker superiorly and not quite reaching the medial cortex.
DIFFERENTIAL DIAGNOSIS None.
DIAGNOSIS Intertrochanteric femur fracture.
DISCUSSION The major fracture line of intertrochanteric fractures extends diagonally from superolateral (greater trochanter) to inferomedial (lesser trochanter). Biomechanical analysis of the fracture suggests a bending movement with the lesser trochanter as the fulcrum, as might occur when stumbling off a curb or falling onto the knee. Most intertrochanteric fractures are comminuted, with the greater and lesser trochanters sometimes present as separate fragments; the lesser trochanter fragment would be the equivalent of a butterfly fragment. Unlike intracapsular femoral neck fractures, these injuries tend to heal promptly and without complication. The incidence of avascular necrosis of the femoral head is about 1%.
Intertrochanteric fractures occur with almost equal frequency in males and females. They occur most frequently in elderly patients older than 75, although they can occur in any age group as a result of massive trauma, such as automobile accidents. Nondisplaced fractures, as seen in this case, are usually two-part in nature and may not be evident on radiographs; even true lateral or oblique views may not show the fracture. MRI is exquisitely sensitive and highly specific in identifying radiographically occult intertrochanteric fractures, and the risk of avascular necrosis as a complication may sometimes be estimated [26,27]. The radionuclide bone scan may not be positive for as many as 4 days [28,29] and is no longer considered an appropriate option in this clinical setting. Treatment consists of open reduction and internal fixation with a dynamic hip screw.
CASE 5.17 CLINICAL HISTORY
A 56-year-old woman with metabolic disease.

FIGURE 5.17
FINDINGS AP radiograph of the pelvis shows osteopenia. The femoral shafts have bowing deformities, and there are horizontal lines with periosteal reactive bone along the medial aspects.
DIFFERENTIAL DIAGNOSIS Osteomalacia, osteoporosis, insufficiency fractures.
DIAGNOSIS Osteomalacia, with Looser’s zones.
DISCUSSION Osteomalacia is the adult manifestation of a systemic disease in which the calcification of osteoid is deficient; the childhood counterpart is rickets. The common final pathway in both conditions is the lack of available calcium or phosphorus (or both) for mineralization of osteoid. In rickets, the predominant effect is on the growth plates; in osteomalacia, the predominant effect is on remodeling of mature bone. Dietary deficiency of vitamin D, usually coupled with inadequate exposure to sunlight so that photochemical synthesis of vitamin D in the skin does not occur, results in reduced gastrointestinal calcium absorption, hypocalcemia, and secondary hyperparathyroidism to mobilize calcium from the skeleton.
Pure vitamin D deficiency-inducedrickets and osteomalacia is relatively rare in the United States, except among immigrants, food faddists, the institutionalized elderly, and patients on total parenteral nutrition. Other causes include failure of enzymatic conversion of 25-hydroxyvitamin D to its physiologically more active metabolite 1,25-dihydroxyvitamin D, end-organ insensitivity to 1,25-dihydroxy vitamin D, genetic and acquired renal tubular reabsorptive defects, and gastrointestinal malabsorption of dietary calcium or phosphorus.
In the United States, gastrointestinal malabsorption from a variety of etiologies is the most common cause of osteomalacia. It may also be caused by chronic use of anticonvulsant medications or of aluminum-containing antacids. In osteomalacia, the radiologic findings are more subtle than in rickets, because the adult skeleton is less metabolically active. Osteopenia is the predominant appearance, and it may be indistinguishable from osteoporosis unless Looser’s zones or bowing deformities are present. Occasionally, the bone texture may be recognized as subtly coarsened. As in osteoporosis, the risk of fractures from trauma escalates with deteriorating bone strength.
CASE 5.18 CLINICAL HISTORY
A young boy with right distal thigh pain for 2 weeks.

FIGURE 5.18A

FIGURE 5.18B

FIGURE 5.18C
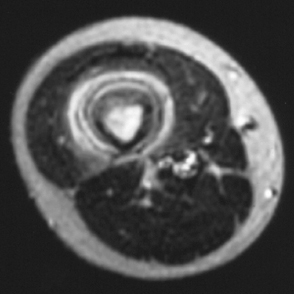
FIGURE 5.18D
FINDINGS
- A, B. Lateral and AP radiographs of the right femur show a region of cortical thickening and sclerosis involving the middle third of the shaft. Smooth periosteal elevation is present in a single layer.
- C. Coronal inversion recovery MRI of both femurs shows a high-signal-intensity abnormality in the right femoral shaft and surrounding edema. The marrow abnormality has a diffuse margin, with the normal marrow in the proximal and distal shaft. The soft tissue abnormality has tapered margins proximally and distally. It appears symmetric and fusiform in morphology.
- D. Axial T2-weighted MRI through the middle of the lesion shows high signal intensity in the medullary space, in the anterior femoral cortex, and in the surrounding soft tissues. The femur is surrounded by a couple of layers of dark periosteal new bone.
DIFFERENTIAL DIAGNOSIS Ewing sarcoma, osteosarcoma, lymphoma, osteomyelitis, stress fracture.
DIAGNOSIS Stress fracture.
DISCUSSION The exquisite sensitivity of MRI to changes in the bone marrow and soft tissues may lead to an overestimation of the aggressiveness and extent of some benign bone lesions, particularly in children [30,31]. Such lesions include chondroblastoma, osteoid osteoma, eosinophilic granuloma (EG), and stress fractures. Commonly seen potentially misleading MRI features include prominent marrow edema, soft tissue edema, and apparent mass effect adjacent to the bone lesion. Features that these lesions have in common that may explain the MRI findings include associated inflammatory reactions caused by the lesions, and their occurrence in childhood, when the periosteum is attached more loosely.
CASE 5.19 CLINICAL HISTORY
A 58-year-old man with recurrent episodes of thigh pain and drainage, separated by decades of good health after a fracture at age 22.

FIGURE 5.19A
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


