ECHOCARDIOGRAPHY: BASIC
AND ADVANCED APPLICATIONS
 INTRODUCTION
INTRODUCTION
The introduction of three-dimensional ultrasound (3-D ultrasound or volume sonography) to obstetric imaging provided an advance in imaging technology. Unlike conventional two-dimensional ultrasound (2-D), 3-D ultrasound provides a volume of a target anatomic region, which contains an infinite number of 2-D planes. The technology of 3-D ultrasound is based on advanced mechanical and electronic transducers with the ability to acquire a volume by a sweep of elements within the transducers and on rapid computer processors able to display the acquired information within milliseconds. The acquired 3-D volume can then be displayed either in a multiplanar format of 2-D images or as a spatial volume projecting the external or internal anatomic features of a volume on the screen. Despite these obvious advances afforded by 3-D sonography, the acquisition, display, and manipulation of 3-D volumes are techniques that require a substantial learning curve. In obstetric sonography, the variable position of the fetus within the uterus further adds to this technical difficulty and limits the clinical applicability of 3-D sonography, especially as it involves complex anatomic structures such as the fetal heart. In this chapter, we will present the basic and advanced principles of 3-D ultrasound as it relates to the examination of the fetal heart. The potential applications of 3-D sonography in the evaluation of fetal cardiac anomalies are shown in the respective chapters on abnormal hearts later in this book.
 THREE-DIMENSIONAL VOLUME ACQUISITION
THREE-DIMENSIONAL VOLUME ACQUISITION
The first step in 3-D volume acquisition is the optimization of the 2-D ultrasound examination, because the quality of the 3-D volume is dependent on the quality of the 2-D ultrasound examination. The operator should ensure optimum 2-D image quality when scanning the fetal heart by following the steps listed in Table 9-1 as acquisition of a 3-D volume initiates from a 2-D ultrasound examination. The term reference plane is used to designate the starting 2-D plane for a 3-D acquisition.
In the commonly used mechanical 3-D transducers, the optimum image quality within a volume is noted in the reference plane and in the parallel planes to the reference plane, whereas the reconstructed orthogonal or oblique planes to the reference plane have a reduced image quality. The reference plane should therefore be chosen based on the anatomic region of interest within the heart. The four-chamber plane is best suited as the 3-D volume reference plane for the evaluation of the transverse planes of the chest including the cardiac chambers, origin of great vessels, and the three-vessel and three-vessel-trachea views. On the other hand, optimal evaluation of the aortic, ductal arches and venous connections is best achieved from a sagittal 3-D volume acquisition of the fetal chest. Acquisitions are also best achieved from a near-ventral approach (spine posterior), avoiding shadowing from the ribs and spine.
Three important considerations should be taken into account when acquiring a 3-D volume: (a) the size of the region of interest (ROI—3-D box), (b) the angle of acquisition, and (c) the resolution or quality of acquisition.
1. ROI box: The ROI determines two parameters of a 3-D volume, the height and width, corresponding to the x and y axes (Fig. 9-1). It is recommended that the operator uses the smallest ROI size that includes all the anatomic components of a target volume. The smallest ROI size that contains all the anatomic components of the fetal heart and its vascular connections will ensure the fastest acquisition while minimizing artifact within the volume.
2. Angle of acquisition: The angle of acquisition is the sweep angle of the elements within the probe and is adjusted by the operator in the 3-D preset prior to the 3-D volume
| TABLE 9-1 | Steps to Optimize the Two-dimensional Ultrasound Examination of the Fetal Heart |

acquisition. The angle of acquisition refers to the depth of a volume, corresponding to the z axis (Fig. 9-1). A basic knowledge of the anatomy of the target organ and the type of acquisition is required when choosing an angle for a 3-D volume. Current options for the acquisition angle of a volume vary from 10 to 120 degrees based on various equipment manufacturers and specific probes. Matrix transducers currently provide limited acquisition angles. Spatio-temporal image correlation (STIC) acquisition angles are typically chosen between 20 and 35 degrees. Static 3-D acquisition angles are between 35 and 45 degrees, which is generally sufficient for the examination of the fetal chest providing anatomic details extending from the stomach inferiorly to the transverse aortic arch (clavicles) superiorly. Ensuring the smallest angle of acquisition of a 3-D volume will enhance the speed of acquisition, reduce artifact, and optimize the quality of the 3-D volume.
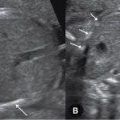
3. Quality of acquisition: The quality of acquisition refers to the number of planes acquired within a volume (Fig. 9-2). In 3-D static acquisition the quality is referred to as low, medium, or high (Fig. 9-2), whereas in STIC acquisition, the quality of acquisition is reflected in the duration of acquisition: 7.5, 10, 12.5, or 15 seconds (Fig. 9-2). The ROI size, acquisition angle, and quality should be adapted based on the type of 3-D volume and the target anatomic region in order to optimize result.

Figure 9-1. Prior to a volume acquisition, the reference plane is chosen by placing a box over the region of interest. The size of the box defines the width (x axis) and height (y axis) of a volume. The acquisition angle of a volume corresponds to its depth (z axis). This figure shows two volume acquisitions with the same width and height but with different depths (acquisition angles). The reference plane (four-chamber view) is located in the middle of the box. It is shown at the front in this figure for better illustration.
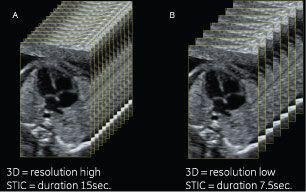
Figure 9-2. Three-dimensional (3-D) volume resolution is dependent on the resolution of the two-dimensional image prior to acquisition and on the number of slices (planes) within the acquisition box. A large number of slices is acquired when resolution is set on high in 3-D static acquisitions (A) and when the duration of acquisition is long in spatio-temporal image correlation (STIC) acquisitions (A). The resolution is set on “low” and the duration is short in B.
The multiplanar display of a 3-D volume provides information on the ROI and the angle of acquisition of the displayed volume. Plane A (left upper) in a multiplanar display corresponds to the reference plane, which is the starting anatomic 2-D plane of a 3-D volume and thus displays the respective size of the ROI in that volume (Fig. 9-3). Plane B (right upper) in a multiplanar display is a reconstructed orthogonal plane to plane A and shows the respective angle of acquisition of that volume (Fig. 9-3). In looking at the multiplanar display of a 3-D volume, one can gauge the appropriateness of the ROI and the angle of acquisition with regard to the target anatomic organ under study (Fig. 9-3). A proposed nomenclature for the clarification of 3-D terms was presented by Deng (1). Current options for 3-D volume acquisition are hereby presented.
Static Three-dimensional (Direct Volume Scan: Nongated)
Principle
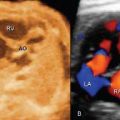
Static 3-D acquisition refers to the acquisition of a 3-D volume in a nongated static mode (Fig. 9-4). The acquired volume contains an infinite number of 2-D still ultrasound planes with no regard to temporal or spatial motion. Currently, this is the most common mode of volume acquisition in obstetrics and gynecology and is frequently used for 3-D evaluation of fetal organs. The four-chamber plane is best used as the reference plane for the static 3-D acquisition when cardiac chambers and the origin of great vessels are under study. For the assessment of aortic or pulmonary arches, reference planes in parasagittal orientation are recommended.
Advantages
Advantages of static 3-D acquisition of the fetal heart include its speed of acquisition (0.5 to 2 seconds) and the ease of volume manipulation. Furthermore, static 3-D acquisition allows for the possibility to acquire large volumes, both in ROI and angle with minimal artifact. The static 3-D acquisition can also be combined with color, power Doppler, or B flow for vascular evaluation of volume content. The authors prefer the use of power Doppler or B flow in static 3-D acquisition given its uniform color display (2–4). Motion artifact is minimized when vessel pulsatility is reduced during volume acquisition with power Doppler (3,5).
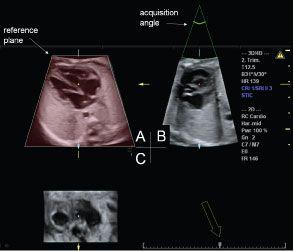
Figure 9-3. Orthogonal display of a spatio-temporal image correlation (STIC) volume acquired at the four-chamber view. The reference plane is depicted in the left upper image (A) with the chosen volume height and width. The acquisition angle 30[degree] is shown in plane B, in the right upper image. Plane B also provides information on acquisition artifacts (motion). The timeline of the STIC volume is shown in the right lower image (C) and the arrow points to the actual time of the orthogonal display within the cardiac cycle. Moving the cursor over the line allows scrolling through systole and diastole.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


