Gestational period between conception and 13 weeks ±5 days
Nomenclature to be used:
Embryo <10 weeks
Fetus >10 weeks until delivery
Pituitary gland secretes FSH and LH, which stimulates the growth of many primary follicles and a dominant (Graffian) follicle in the ovary due to estrogen stimulation.
Just before ovulation, progesterone and LH surge leads to formation of corpus luteum.
Corpus luteum secretes progesterone. If there is no pregnancy, corpus luteum involutes.
If pregnancy is positive, hCG maintains the corpus luteum and progesterone is responsible for decidual reaction.
Corpus luteum is the most common finding noted in the first trimester. Progesterone supports the pregnancy until the placenta can take over its hormonal process. May regress around 16–18 weeks of gestational age (GA).
Human chorionic gonadotropin (hCG) is a glycoprotein secreted by the outer layer of cells of gestation or chorionic sac (syncytiotrophoblasts). Negative hCG excludes the presence of live pregnancy. Beta-hCG levels in normal pregnancy can be detected about 11 days after conception by a blood test and 12–14 days after conception by a urine test. It has a doubling time of approximately 2–3 days. hCG levels begin to rise, reaching up to an average peak of 100,000 international units per liter; in the first 8–11 weeks of pregnancy.
Low levels suggest miscalculated dates, possible miscarriage, and ectopic pregnancy.
High levels suggest wrong dates, molar, and multiple pregnancies.
1. To identify the location and the number of the gestational sac (GS)
2. To assign a GA to the pregnancy
3. To evaluate normal early pregnancy
4. To look for any sonography indicators predicting failure
5. To assess maternal symptoms such as pain or bleeding
6. To evaluate uterine contents before the termination of pregnancy
7. To guide diagnostic/therapeutic procedures
USG APPEARANCES OF A NORMAL I/U GESTATION
First USG sign to suggest early pregnancy.
Implantation commonly occurs in the fundal region of uterus between the 20th and 23rd day.
25–29 days of menstrual age (b-hCG +ve)→ Intradecidual sign (Small gestation sac within the decidua/focal echogenic thickening of endometrium at the site of implantation).
4.5–5 weeks menstrual age—Intradecidual sac (Normal GS).
Threshold level: Earliest we can expect to see a sac 4 weeks 3–4 days.
Discriminatory level: We should always see the sac at 5 weeks 3 days (Table 17.1).
GA | GS | YS | Embryo | Heart heat |
5 weeks | + | − | − | − |
5.5 weeks | + | + | − | − |
6.0 weeks | + | + | + | + |
DOUBLE DECIDUAL SAC SIGN (INTERDECIDUAL) (FIGURE 17.1A)
It is based on visualization of three layers of decidua in early pregnancy. There are two concentric echogenic rings surrounding a portion of GS.
Ring closest to the sac—Smooth chorion laeve and decidua capsularis.
Ring peripherally located—Decidua vera (echogenic endometrial lining).
Present when MSD >10 millimeters at 5–6 weeks GA.
Decidua basalis—Chorion frondosum forms future placenta—Seen as an area of eccentric echogenic thickening.
On TAS at 5½ weeks, two blebs represent the amnion and yolk sac (YS).
Thin amniotic membrane divides amniotic and coelomic cavity.
Amniotic fluid fills in the amniotic cavity, which grows faster than the chorionic cavity and by 16 weeks, amniotic membrane is not seen as a separate structure.
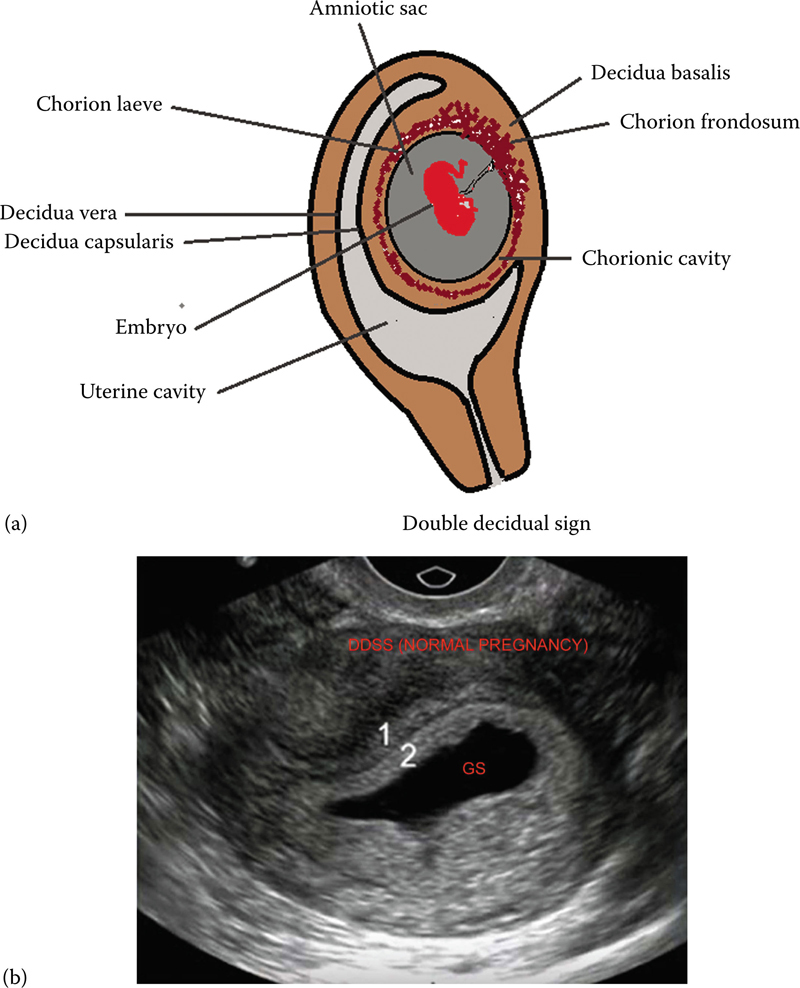
Figure 17.1 (a) Illustrates double decidual sac sign (DDSS) and (b) illustrating two concentric rings of normal pregnancy.
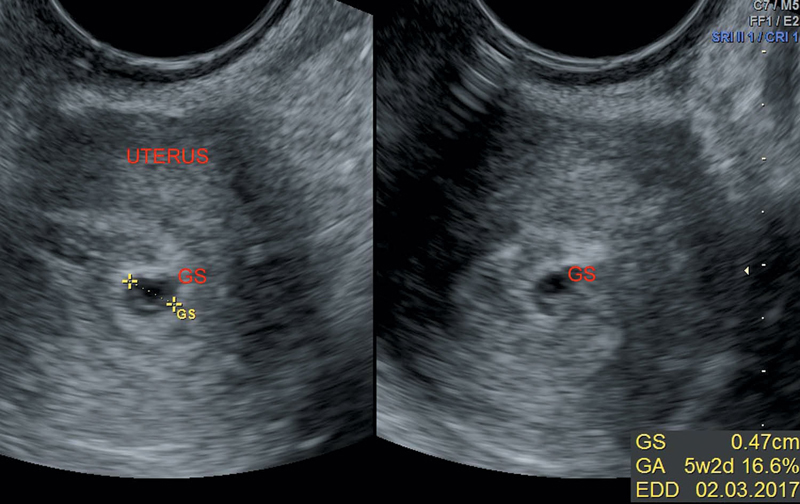
Figure 17.2 Illustrating small anechoic G sac in early pregnancy.
Small round fluid collection surrounded by echogenic rim of tissue (Figure 17.2).
Normally, gestation sac is round in very early stages. As it enlarges, it has oval shape d/t pressure exerted by muscular uterine walls.
Calculated by adding three orthogonal dimensions of the chorionic cavity (excluding the surrounding echogenic rim) and divided by three.
First structure seen normally within the gestation sac, confirmatory of intrauterine pregnancy.
Round lucent structure with echogenic periphery, located in chorionic cavity outside the amniotic membrane (Figures 17.3 and 17.4).
Helps in
• Transfer of nutrients to the embryo
• Angiogenesis
• Hematopoesis
Using TAS: YS always seen with MSD of 20 millimeters
Using TVS: YS always seen with MSD of 8 millimeters
Number of YSs help in determining the amnionicity of the pregnancy.
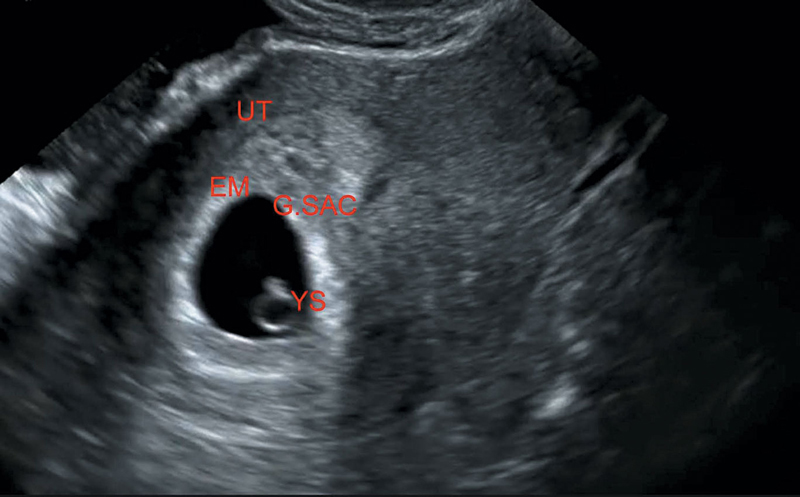
Figure 17.3 Illustrating yolk sac in early pregnancy.
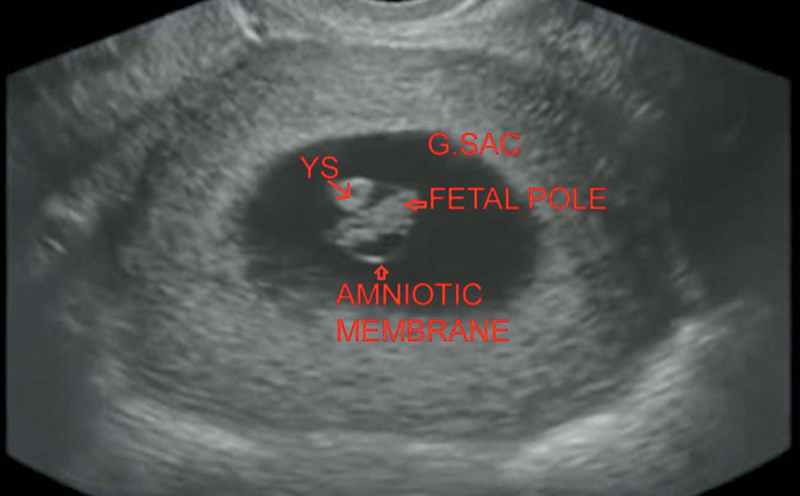
Figure 17.4 Illustrates early intrauterine pregnancy at around 7 weeks.
MCMA—Two embryos, one chorionic sac, one amniotic sac, and one YS.
DCDA—Two embryos, two chorionic sac, two amniotic sac, and two YS.
YS remains connected to the midgut by the vitelline duct (Omphalomesenteric duct [OMD]).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


