A variable effectiveness of reparative and recovery mechanisms following tissue damage is among the factors that might contribute to explaining resolution of symptoms and maintenance of a normal level of function in patients who have multiple sclerosis (MS). The application of functional MR imaging in MS has shown that cortical changes do occur after white matter injury and that these changes can contribute to limiting the clinical outcome of such damage. Conversely, the failure or exhaustion of the adaptive properties of the cerebral cortex with increasing disease duration and burden might be among the factors responsible for the accumulation of fixed neurologic deficits in patients who have MS.
Over the past decade, conventional and modern structural MR imaging techniques have been extensively used to study patients who have multiple sclerosis (MS) with the ultimate goal of increasing the understanding of the mechanisms responsible for the accumulation of irreversible disability. In summary, the application of MR imaging techniques to the definition of MS pathophysiology has shown that: (1) MS-related damage is not restricted to T2-visible lesions, but it involves diffusely the normal-appearing white matter (NAWM) and gray matter (GM); (2) the neurodegenerative component of the disease is not a late phenomenon and it is not fully driven by inflammatory demyelination; and (3) axonal damage contributes significantly to the clinical manifestations of the disease. Despite this, however, the magnitude of the correlation between MR imaging and clinical findings remains suboptimal.
Among the reasons for such a discrepancy, a variable intra- and intersubject effectiveness of reparative and recovery mechanisms following MS-related tissue injury is increasingly being considered. In this context, brain plasticity, a well-known feature of the human brain, which is likely to result from the interplay of several different substrates (such as increased axonal expression of sodium channels, synaptic rearrangement, increased recruitment of parallel existing pathways or “latent” connections, and reorganization of distant sites), is viewed as a major factor with an adaptive role in limiting the functional outcome of axonal loss in MS.
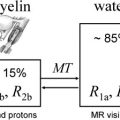
The signal changes seen during functional MR (fMR) imaging studies depend on the blood oxygen level–dependent (BOLD) mechanism, which, in turn, involves changes of the transverse magnetization relaxation time—either T2 ∗ in a gradient echo sequence, or T2 in spin echo sequence. Local increases in neuronal activity result in an increase of blood flow and oxygen consumption. The increase of blood flow is greater than the oxygen consumption, thus determining an increased ratio between oxygenated and deoxygenated hemoglobin, which enhances the MR imaging signal.
This article summarizes the main contributions to the understanding of MS pathobiology gained by the use of fMR imaging with different paradigms of stimulation.
General considerations
The main problem in the interpretation of fMR imaging studies in diseased people is that the observed changes might be biased by disease-driven differences in task performance between patients and controls. Clearly, this is a major issue in MS, which typically causes impairment of various functional systems. Despite providing several important pieces of information, therefore, the value of the earliest fMR imaging studies of patients who have MS has to be weighed against this background. For this reason, the most recent fMR imaging studies in MS have been based on larger and more selected patient groups than the seminal studies. These latter studies have investigated the brain patterns of cortical activations during the performance of several motor, visual, and cognitive tasks in patients who have all the major clinical phenotypes of the disease. One of the most solid conclusions that can be drawn from fMR imaging studies of MS is that cortical reorganization does occur in patients affected by this condition. The correlation between various measures of structural MS damage and the extent of cortical activations also suggests an adaptive role of such cortical changes in contributing to clinical recovery and maintaining a normal level of functioning in patients who have MS, despite the presence of axonal/neuronal loss, and, conversely, their failure or exhaustion with increasing disease duration or burden is likely to contribute to the accrual of irreversible disability.
The visual system
The method usually applied to investigate the visual system in MS and related disorders consists of the application of an 8 Hz photic stimulation to one or both eyes.
Acute Optic Neuritis Suggestive of Multiple Sclerosis
Compared with healthy controls, patients who have recovered from a single episode of acute unilateral optic neuritis, when the clinically affected eye is studied, show an extensive activation of the visual network, including the claustrum, lateral temporal and posterior parietal cortices, and thalamus, in addition to the primary visual cortex. When the unaffected eye is stimulated, only activations of the visual cortex and the right insula/claustrum are observed. In addition, the volume of the extra-occipital activation is strongly correlated with the latency of the visual evoked potential (VEP) P100, suggesting that the functional reorganization of the cortex might represent an adaptive response to a persistently abnormal visual input.
Subsequent studies have confirmed the results of this seminal report. Toosy and colleagues used a longer photic stimulation epoch to better elucidate the nature of the abnormal extra-occipital response, which had a peak during the OFF phase of the stimulation paradigm. The results of this study confirm the original finding of a phase-dependent increase of the BOLD signal in the extra-occipital regions during the baseline condition. Russ and colleagues used fMR imaging and VEP to monitor the functional recovery after an acute unilateral optic neuritis and found a strong relationship between fMR imaging and VEP latencies, suggesting that fMR imaging can contribute to the assessment of the temporal evolution of the visual deficits during recovery, either natural or modified by treatment. Levin and colleagues showed reduced activation of the primary visual cortex and increased activation of the lateral occipital complex (LOC) in eight subjects who recovered clinically from an episode of optic neuritis, but who still had prolonged VEP latencies in comparison with healthy controls. More recently, in a 1-year follow up study, Toosy and colleagues, using a novel technique that modeled the fMR imaging response and optic nerve structure together with clinical function, demonstrated a potential adaptive role of cortical reorganization within the extrastriate visual areas, which are regions involved in higher-order visual processing, early after optic neuritis. In addition, at 3 months more severe optic nerve damage was associated with an increased fMR imaging response in the bilateral temporal cortices, whereas at 1 year, the right temporal cortex correlation reversed. These results illustrate how the same regions may play different roles at different times during recovery, reflecting the complexity of brain plasticity and the demyelinating process. This notion has been supported by a recent region-of-interest longitudinal study that demonstrated dynamic changes of the fMR imaging response following visual stimulation not only in V1, V2, and the LOC, but also in the lateral geniculate nucleus (LGN) in patients who had isolate acute optic neuritis ( Fig. 1 ).
Relapsing-Remitting Multiple Sclerosis
In patients who had established MS and a relapsing-remitting (RR) course with a unilateral optic neuritis, a reduced recruitment of the visual cortex after stimulation of the affected and the unaffected eyes was found when compared with healthy subjects. On average, patients who had complete clinical recovery showed a greater visual cortex recruitment than those who had poor or no recovery, although the extent of the activation remained reduced compared with that of controls. A more recent study of nine patients who had a previous optic neuritis showed that these patients not only have a reduced activation of the V1, but also a reduced fMR imaging percentage signal change in this region, again suggesting an abnormality of the synaptic input.
The visual system
The method usually applied to investigate the visual system in MS and related disorders consists of the application of an 8 Hz photic stimulation to one or both eyes.
Acute Optic Neuritis Suggestive of Multiple Sclerosis
Compared with healthy controls, patients who have recovered from a single episode of acute unilateral optic neuritis, when the clinically affected eye is studied, show an extensive activation of the visual network, including the claustrum, lateral temporal and posterior parietal cortices, and thalamus, in addition to the primary visual cortex. When the unaffected eye is stimulated, only activations of the visual cortex and the right insula/claustrum are observed. In addition, the volume of the extra-occipital activation is strongly correlated with the latency of the visual evoked potential (VEP) P100, suggesting that the functional reorganization of the cortex might represent an adaptive response to a persistently abnormal visual input.
Subsequent studies have confirmed the results of this seminal report. Toosy and colleagues used a longer photic stimulation epoch to better elucidate the nature of the abnormal extra-occipital response, which had a peak during the OFF phase of the stimulation paradigm. The results of this study confirm the original finding of a phase-dependent increase of the BOLD signal in the extra-occipital regions during the baseline condition. Russ and colleagues used fMR imaging and VEP to monitor the functional recovery after an acute unilateral optic neuritis and found a strong relationship between fMR imaging and VEP latencies, suggesting that fMR imaging can contribute to the assessment of the temporal evolution of the visual deficits during recovery, either natural or modified by treatment. Levin and colleagues showed reduced activation of the primary visual cortex and increased activation of the lateral occipital complex (LOC) in eight subjects who recovered clinically from an episode of optic neuritis, but who still had prolonged VEP latencies in comparison with healthy controls. More recently, in a 1-year follow up study, Toosy and colleagues, using a novel technique that modeled the fMR imaging response and optic nerve structure together with clinical function, demonstrated a potential adaptive role of cortical reorganization within the extrastriate visual areas, which are regions involved in higher-order visual processing, early after optic neuritis. In addition, at 3 months more severe optic nerve damage was associated with an increased fMR imaging response in the bilateral temporal cortices, whereas at 1 year, the right temporal cortex correlation reversed. These results illustrate how the same regions may play different roles at different times during recovery, reflecting the complexity of brain plasticity and the demyelinating process. This notion has been supported by a recent region-of-interest longitudinal study that demonstrated dynamic changes of the fMR imaging response following visual stimulation not only in V1, V2, and the LOC, but also in the lateral geniculate nucleus (LGN) in patients who had isolate acute optic neuritis ( Fig. 1 ).
Relapsing-Remitting Multiple Sclerosis
In patients who had established MS and a relapsing-remitting (RR) course with a unilateral optic neuritis, a reduced recruitment of the visual cortex after stimulation of the affected and the unaffected eyes was found when compared with healthy subjects. On average, patients who had complete clinical recovery showed a greater visual cortex recruitment than those who had poor or no recovery, although the extent of the activation remained reduced compared with that of controls. A more recent study of nine patients who had a previous optic neuritis showed that these patients not only have a reduced activation of the V1, but also a reduced fMR imaging percentage signal change in this region, again suggesting an abnormality of the synaptic input.
Motor system
The investigation of the motor system in patients who have MS has mainly focused on the analysis of the performance of simple motor tasks with the dominant right upper limbs. Such tasks were either self-paced or paced by a metronome. A few studies assessed the performance of simple motor tasks with the dominant right lower limbs, and even fewer studies have investigated the performance of more complex tasks, including phasic movements of dominant hand and foot, object manipulation, and visuomotor integration tasks.
Clinically Isolated Syndromes Suggestive of Multiple Sclerosis
An altered brain pattern of movement-associated cortical activations, characterized by an increased recruitment of the contralateral primary sensorimotor cortex (SMC) during the performance of simple tasks and by the recruitment of additional classic and higher-order sensorimotor areas during the performance of more complex tasks has been demonstrated in patients who have clinically isolated syndromes (CIS) suggestive of MS. The clinical and conventional MR imaging follow-up of these patients has shown that, at disease onset, patients who have CIS with a subsequent evolution to clinically definite MS tend to recruit a more widespread sensorimotor network than those who do not have short-term disease evolution. These findings support the notion that, although increased recruitment of a widespread sensorimotor network contributes to limiting the impact of structural damage during the course of MS, its early activation might be counterproductive, because it might result in an early exhaustion of the adaptive properties of the brain.
Relapsing-Remitting Multiple Sclerosis
An increased recruitment of several sensorimotor areas, mainly located in the cerebral hemisphere ipsilateral to the limb that performs the task, has been demonstrated in patients who have early RRMS and a previous episode of hemiparesis. In patients who had similar characteristics, but who presented with an episode of optic neuritis, this increased recruitment involved sensorimotor areas that were mainly located in the contralateral cerebral hemisphere.
In patients who have RRMS, functional cortical changes, mainly characterized by an increased recruitment of classic motor areas, including the primary SMC, the supplementary motor area (SMA), and the secondary sensorimotor cortex (SII), have been shown during the performance of simple motor and visuomotor integration tasks. More recently, abnormal functional connectivity of the motor network has also been demonstrated to occur in these patients.
Progressive Multiple Sclerosis
Movement-associated cortical changes, characterized by the activation of highly specialized cortical areas, have been described in patients who have secondary progressive (SP) MS during the performance of a simple motor task and in patients who have primary progressive (PP) MS during the performance of active and passive motor experiments.
Cognition
Recent fMR imaging studies have suggested that functional cortical changes might have an adaptive role also in limiting MS-related cognitive impairment. Several cognitive domains have been investigated in patients who have MS with fMR imaging. Working memory has been the most extensively studied by using the Paced Auditory Serial Addition Test (PASAT) or the Paced Visual Serial Addition Task (PVSAT) (which also involves sustained attention, information processing speed, and simple calculation), the n-back task, or a task adapted from the Sternberg paradigm. Additional cognitive domains including attention and planning have also been interrogated.
Clinically Isolated Syndromes Suggestive of Multiple Sclerosis
In patients who have CIS, an altered pattern of cortical activations has been described during the performance of the PASAT, confirming the presence of cortical reorganization at the earliest clinical stage of the disease.
Relapsing-Remitting Multiple Sclerosis
During the performance of the PVSAT, patients who have RRMS with a preserved task performance have increased activations of several regions located in the frontal and parietal lobes, bilaterally. Similarly, cognitively preserved RRMS showed, during an n-back test, a reduced activation of the core areas of the working memory circuitry (including prefrontal and parietal regions) and an increased recruitment of other regions within and beyond the typical working memory circuitry (including areas in the frontal, parietal, temporal and occipital lobes). An increased recruitment of several cortical areas (in particular in the frontal and temporal lobes) has also been shown in patients who have RRMS and mild clinical disability during the performance of a simple cognitive task, and when testing rehearsal within working memory. In this latter case, the degree of right hemisphere recruitment was strongly related to the neuropsychologic performance. Other studies, which also investigated working memory, demonstrated that compared with controls, patients who have MS have (1) an increased recruitment of regions related to sensorimotor functions and anterior attentional/executive components of the working memory system, and (2) a reduced activation of several regions in the right cerebellar hemisphere.
A recent fMR imaging study applied an analysis of functional connectivity to investigate n-back functional correlates in a group of 21 patients who had RRMS. Compared with controls, patients had relatively reduced activations of the superior frontal and anterior cingulate gyri, and a smaller increase of activation with greater task complexity. This finding suggests a reduced functional reserve for cognition relevant to memory in these patients. In addition, the analysis of functional connectivity revealed increased correlations between right dorsolateral prefrontal and superior frontal/anterior cingulate activations in controls, and increased correlations between activations of the right and left prefrontal cortices in patients. This finding suggests that an altered interhemispheric interaction between dorsal and lateral prefrontal regions may yet be an additional adaptive mechanism distinct from recruitment of novel processing regions.
Benign Multiple Sclerosis
Using a 3.0 T scanner, more significant activations of several areas of the cognitive network involved in the performance of the Stroop test have been demonstrated in cognitively preserved patients who have benign MS (BMS) ( Fig. 2 ). Patients who had BMS also showed an increased connectivity between several cortical areas of the cognitive network (including the left and right inferior frontal gyri [IFG], the anterior cingulate cortex, and the left SII), and between some of these areas and the right cerebellum, and a decreased connectivity between some other areas (including the left SII, the prefrontal cortex, and the right cerebellum) and the anterior cingulate cortex. These results suggest an altered interhemispheric balance in favor of the right hemisphere in patients who have BMS in comparison with healthy controls, when performing cognitive tasks.