Functional Renal Anatomy, Renal Physiology, and Contrast Media
Functional Renal Anatomy, Renal Physiology, and Contrast Media
FUNCTIONAL RENAL ANATOMY
The kidney maintains the homeostasis of body fluids through the excretion of metabolic end products and toxins, the regulation of body fluid volume and blood pressure, and the regulation of mineral and acid-base balance. While the regulatory function of the kidney directly affects the one-third of the fluid that is located in the vascular compartment, because there is free movement of water between the intracellular and extracellular fluid (ECF) compartments, the latter containing two-thirds of the body fluid volume, renal function actually affects the composition of all body fluids.
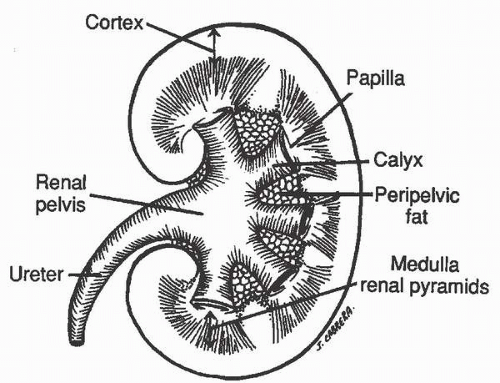
The kidney consists of (1) an inner renal medulla and (2) an outer renal cortex (Fig. 2.1). The functional unit of the kidney is the nephron (Fig. 2.2). Each kidney contains approximately 1 million nephrons. Each nephron consists of a specialized capillary vascular network called the glomerulus, which is surrounded by Bowman capsule, a balloon-like structure into which the capillary tufts of the glomerulus protrude. Each glomerulus is connected to a series of specialized epithelial segments that collectively are known as the renal tubule.
FIGURE 2.1. Bisected section of the kidney showing the relationship of the cortex, the medulla, and the renal collecting system. Fat in the renal sinus surrounds the calyces and the renal pelvis.
FIGURE 2.2. The nephron. G, glomerulus; TAL, thick ascending limb of the loop of Henle; tAL, thin ascending limb of the loop of Henle; PST, proximal straight tubule; PCT, proximal convoluted tubule; DCT, distal convoluted tubule; tDL, thin descending limb of loop of Henle; CCD, cortical collecting duct; MCD, medullary collecting duct; PCD, papillary collecting duct; VR, vasa recta.
The tubule is divided into several segments. The first segment, the proximal tubule, is subdivided into convoluted and straight portions; the second segment, the loop of Henle, is subdivided into the thin descending, the thin ascending, and the thick ascending limbs; and the third segment, the distal tubule, is subdivided into the distal convoluted tubule and the cortical, medullary, and papillary collecting ducts. The renal cortex contains the glomeruli, the proximal tubule, the distal tubule, and the cortical collecting duct. The renal medulla is made up of the loops of Henle, the medullary and papillary collecting ducts, and renal pyramids, the apices of which project into the minor calyces. The nephrons that are located close to the corticomedullary junction have larger glomeruli, and their loops of Henle descend deeper into the renal papilla than those located more superficially in the renal cortex.
The main renal artery branches into interlobar arteries that divide into the arcuate arteries located at the corticomedullary junction. These, in turn, become the interlobular arteries that finally divide into the afferent arterioles, each of which leads to a glomerulus. The glomerulus is drained by an efferent arteriole that subdivides to form a peritubular capillary network known as the vasa recta. The vasa recta then anastomose to form venous channels. This unique arrangement in the kidney, in which the glomerulus is located between two resistive capillary networks as opposed to the arteriole-capillary-venule arrangement of the other tissues of the body, helps to maintain constant hydrostatic pressure at the level of the glomerulus despite changes in blood pressure and is the driving force for glomerular filtration.
The macula densa is a distinctive portion of the tubule between the ascending loop of Henle and the distal convoluted tubule that courses between the afferent and efferent arterioles. It represents the tubular component of a specialized area of the nephron called the juxtaglomerular apparatus. The juxtaglomerular apparatus is the site of renin synthesis and plays a major role in blood pressure regulation.
BASIC RENAL PHYSIOLOGY
The homeostatic functions of the kidney are achieved through two simultaneous processes: (1) glomerular filtration and (2) tubular resorption/secretion. The net filtration pressure (NFP) is equal to the sum of the glomerular hydrostatic pressure and the colloid osmotic pressure in Bowman capsule (which favors fluid movement from the capillary space into Bowman space) minus the sum of the mean glomerular capillary oncotic pressure and the hydrostatic pressure in Bowman space (the principal forces opposing ultrafiltration). Because protein is not filtered by the glomerulus, the fluid of Bowman space is protein free; thus, the colloid osmotic pressure in Bowman space is negligible. The glomerular filtration rate (GFR) is determined by the NFP and the surface area available for filtration, as well as by the permeability of the glomerular capillary bed. The average GFR in a human with normal renal function is approximately 125 mL/min, which is equal to 180 L/day or approximately 12 times the volume of the ECF.
Although 180 L of fluid is filtered in a day, only 1 to 2 L of urine is produced per day in which wastes may be concentrated 100- to 200-fold above their plasma concentration. This concentration of the final urine product is the result of a combination of tubular secretion and reabsorption. Under normal conditions, approximately two-thirds of the ultrafiltrate volume is reabsorbed in the proximal tubule by a process linked to the active secretion of hydrogen ions and the active reabsorption of sodium, glucose, amino acids, and other solutes. Isotonicity of the fluid in the proximal tubule with the plasma is maintained because the cells of the proximal tubule are freely permeable to water.
In the loop of Henle, which begins at the corticomedullary junction, differential absorption of sodium chloride occurs so that the fluid in the tubular lumen, initially isotonic with the interstitium, becomes progressively more concentrated in the descending limb, reaching its maximum concentration at the bend of the loop and then becomes progressively more hypotonic with respect to plasma as it reaches the thick ascending limb of the loop. This differential absorption of sodium chloride occurs because the cells in the descending limb have a high permeability for water but a low permeability for salt, whereas in the thick ascending limb, the cells are impermeable to water but have a high permeability for salt, which is actively reabsorbed. This process, known as the renal countercurrent mechanism, results in progressive interstitial hypertonicity in the medulla and is required for final concentration of the urine by the distal tubules.
The distal tubule continues the water dilution of urine through the active transport of sodium and chloride coupled with relative water impermeability. The collecting ducts are the primary site of action of antidiuretic hormone (ADH). The final 15% of water absorption is achieved within the collecting ducts. The collecting ducts are virtually impermeable to water in the absence of ADH, but when ADH is present, water passes freely across the tubular wall, allowing the tubular fluid to achieve the same tonicity as the fluid in the surrounding interstitium. Thus, hypertonic urine is produced without the active transport of water. The distal nephron also reabsorbs sodium and secretes hydrogen ions and potassium under the influence of aldosterone. Parathyroid hormone also acts on the distal tubule to conserve calcium.
The rate at which a substance is removed from the plasma in a given period is termed the clearance of that substance. For a substance that is freely filtered and not reabsorbed or secreted by the tubule, the rate of clearance is equal to the GFR. The polysaccharide, inulin, meets this requirement and, therefore, can be used to determine GFR. Creatinine, an endogenous product of muscle metabolism, is produced in relatively constant amounts each day. Creatinine is present in the plasma, and is excreted by glomerular filtration. Measurement of creatinine clearance is therefore convenient, although it is not as exact as the inulin clearance, because a small amount of creatinine is also secreted by the tubules. Because creatinine clearance tends to underestimate renal dysfunction, particularly with mild impairment, the National Kidney Foundation has suggested that the estimated glomerular filtration rate (eGFR) may be a better model for predicting renal dysfunction than relying solely on serum creatinine determinations. eGFR is generally calculated from the serum creatinine by either the Cockcroft-Gault formula or, more commonly, one of the modified diet in renal disease (MDRD) formulae. All of these formulae are calculated using a combination of the serum creatinine level, patient age, and patient gender. The Cockcroft-Gault formula also utilizes patient weight, while the MDRD formulae also accounts for patient race.
The most common of the abovementioned eGFR estimation formulae is the 4-variable MDRD formula, which is listed as follows: eGFR (mL/min/1.73 m2) = 175 × [serum creatinine (µmol/L) × 0.0113]-1.154 × age (years)-0.203 (× 0.742 if female). There are many eGFR calculators available on the Internet.
CONTRAST MEDIA: HISTORICAL BACKGROUND
Although attempts at radiography of the urinary tract began shortly after Roentgen’s discovery in 1895, the first report of opacification of the urinary tract was in 1923, when researchers at the Mayo Clinic discovered opacification of the bladder in patients being treated with sodium iodide. It is remarkable that in the more than 80 years since this discovery, no intravascular element other than iodine has proven suitable for imaging with x-rays.
Attempts at developing an injectable radiopaque iodinated contrast media were initially made in Germany under the direction of Moses Swick, an American urologist, who ultimately focused on linking the iodine to a 6-carbon benzene ring in an attempt to increase water solubility and decrease toxicity.
In 1955, Hoppe et al. at Sterling Winthrop Research Institute produced sodium diatrizoate (Fig. 2.3), a fully substituted derivative of 2,4,6-triiodobenzoic acid, which became the first modern iodinated contrast media. This agent was ionic in that the anionic benzene cation had to be conjugated with a positively charged sodium (cation), with the sodium diatrizoate molecule dissociating into two particles in solution (ratio of three iodine atoms to two particles in solution). This product and its derivatives, including sodium/meglumine diatrizoate and meglumine iothalmate, became the standard urographic contrast media for the next 30 years.
Although these ionic contrast media, which are still commonly used for enteric procedures today, including cystograms, some esophagograms, and some enemas, were safer than the previously used materials, much of the remaining toxicity of the compounds was related to their high osmolality (>1,500 mOsm/kg of water or approximately five times greater than plasma at standard contrast concentrations).
In 1968, Torsten Almen of Malmö, Sweden, theorized that the high osmolality of ionic contrast (with osmolality basically being a measure of the number of particles in solution) could be reduced by synthesizing a product that would be nondissociating. He demonstrated that the ionizing carboxyl group of conventional contrast media could be replaced with a nondissociating hydrophilic group such as an amide, resulting in a ratio of three iodine atoms per one particle in solution. This would theoretically decrease the osmolality by 50%, reducing the number of particles in solution without loss of iodine content. The first nonionic contrast media, metrizamide, was never used in the United States as a urographic agent, because of its considerable cost and the necessity to package it as a freeze-dried lyophilized powder that needed to be reconstituted with water immediately before use.
FIGURE 2.3. Sodium diatrizoate (Hypaque).
Several years after the introduction of metrizamide, second-generation low-osmolality contrast media were introduced into clinical practice. These products developed along two general lines. In the first group, hydrophilic nonionizing radicals were again introduced in positions one, three, and five of the benzene ring, whereas, positions two, four, and six remained the position of the iodine atoms. Because the radical at position number one did not dissociate, the number of iodine atoms relative to the number of particles in solution remained 3:1 rather than 3:2, as noted with ionic contrast media. Compounds in this category, which remain widely used today, include iohexol (Fig. 2.4; Omnipaque; GE Healthcare Inc., Princeton, NJ), iopamidol (Fig. 2.5; Isovue; Bracco Diagnostics Inc., Monroe, NJ), iopromide (Ultravist, Bayer Health Care, Wayne, NJ), and ioversol (Fig. 2.6; Optiray; Mallinckrodt Imaging, Hazelwood, MO). All of these products are generically known as nonionic monomers. Studies have demonstrated that the incidence of adverse events is greatly reduced (by a factor of about five) when nonionic monomers are injected intravenously, in comparison to ionic monomers, a difference that is likely the result of their lower osmolality.
FIGURE 2.4. Iohexol (Omnipaque).
FIGURE 2.5. Iopamidol (Isovue).
FIGURE 2.6. Ioversol (Optiray).
FIGURE 2.7. Iodixanol (Visipaque).
The second line of development of low osmolality contrast was directed toward the linkage of two triiodinated benzene rings together sharing only one ionizing carboxyl group (at position one of one of the benzene rings). These compounds have a ratio of six iodine atoms to two molecules in solution and also produce a ratio of 3:1. These contrast particles are generally known as ionic dimers and have a similar osmolality to nonionic monomers.
Further development involved the linkage of two nonionic monomeric compounds to form a nonionic dimer, which has a ratio of six iodine atoms to one particle in solution, and, therefore, has a ratio of 6:1. This modification has further reduced the osmolality of the resulting contrast media, such that nonionic dimers have an osmolality equal to plasma. Iodixanol (Fig. 2.7; Visipaque; GE Healthcare, Princeton, NJ) is the only one of these agents to be approved for use in the United States. Interestingly, the incidence of acute adverse events after nonionic dimer injection has not been seen to be significantly lower than that encountered after nonionic monomer injection.
Another property of contrast media is viscosity. This property describes the relative adhesiveness of the molecules of the contrast media for one another and is important because the viscosity of the contrast determines how rapidly the contrast may be injected. In general, more concentrated solutions of contrast material are more viscous than less concentrated solutions. Also, larger molecules tend to have higher viscosity than smaller molecules at the same concentrations. So, it is not surprising that nonionic dimers are considerably more viscous than are nonionic monomers. The viscosity of contrast media decreases with increasing temperature. For this reason, warming of viscous contrast material makes injection easier.
PHYSIOLOGY OF CONTRAST EXCRETION
Principles
The currently used triiodobenzoic acid derivative contrast media are excreted by glomerular filtration without significant tubular secretion. After intravenous injection of contrast media, there is a rapid increase followed by a rapid decrease in plasma concentration of contrast media. Although most (88%) of the rapid decline is due to equilibration of the contrast material throughout the ECF, 12% of the decrease in contrast media concentration is due to excretion of the contrast media by the kidneys into the renal collecting systems and ureters. During this period, filtration of the contrast media is at its maximum. Therefore, it is within the first few moments after injection that the nephrogram, representing contrast media within the renal tubules, is at its peak intensity.
The degree of opacification of the urinary tract is not a function of the concentration of the contrast media in the urine alone, but it is the total amount of contrast media (urinary contrast concentration times the volume of urine produced) on which opacification depends. Thus, opacification depends on the total number of iodine atoms in the path of the x-ray beam rather than on their concentration in the urine. There is also a dose-related increase in the urine flow rate that occurs after contrast media administration, which is related to the fact that monomeric contrast media acts as an osmotic diuretic.
The rate of excretion of contrast media is greatest in the first 10 minutes after injection and falls logarithmically thereafter. With increasing time, the contrast media that had equilibrated with the ECF returns to the vascular space and is excreted. Approximately 24 hours is required to excrete 100% of the administered dose (Fig. 2.8).
The sequential change in the computed tomography (CT) attenuation value for the renal cortex that occurs after bolus administration of contrast media intravenously directly correlates with the amount of iodine administered. Indeed, a plot of CT number against time (Fig. 2.9) produces a curve similar in appearance to the plot of plasma contrast concentration against time. Therefore, the change in CT number in the renal cortex following contrast media administration accurately reflects the physiology of contrast media excretion.
Physiologic Considerations
In the past, overnight fluid restriction was often recommended to improve the diagnostic quality of excretory urography, by increasing the concentration and, thereby, the radiopacity of excreted contrast material in the renal collecting systems and ureters. The rationale of this approach was based on the physiologic principle that in a dehydrated state, ADH production is stimulated and results in more concentrated urine. Fluid restriction is not needed prior to performance of CT or MRI, however, and, in fact, is discouraged. Overhydration may have an adverse effect on pyelographic density on CT or MRI in patients being hydrated with intravenous fluids. A “washout” of the pyelogram can occur if excretory phase CT is to be performed, although the quality of the nephrogram is usually unaffected. There is, however, no evidence that diagnostic accuracy is compromised by the reduced concentration of excreted contrast material in the renal collecting systems and ureters of these patients.
FIGURE 2.8. Graph demonstrating cumulative excretion of Hypaque. (From Cattell WR, Fry IK, Spencer AG, et al. Excretory urography 1-factors determining the excretion of Hypaque. Br J Radiol. 1967;40(476):561-571.)
FIGURE 2.9. The sequential change in CT numbers measured in the renal cortex following an acute injection of contrast material shows a rapid decline. (From Brennan RE, Curtis JA, Pollack HM, et al. Sequential changes in the CT numbers of the normal canine kidney following intravenous contrast administration. I. The renal cortex. Invest Radiol. 1979;14(2):141-148.)
Phases of Contrast Enhancement on CT and MRI
On CT and MRI, four phases of contrast enhancement have been described: (1) an arterial phase, during which time abdominal arterial enhancement is highest, generally occurring at 20 to 40 seconds after initiation of contrast material injection; (2) a corticomedullary phase, at which time the arterial concentration decreases, but when there is a maximal difference in attenuation between hyperenhancing renal cortex and hypoenhancing renal medulla (peaking in most patients at 60 to 70 seconds after the contrast injection begins; (3) a nephrographic phase, during which time the renal cortex and medulla enhance similarly, resulting in renal parenchymal homogeneity, usually occurring at 90 to 120 seconds); and (4) an excretory phase, which begins with the appearance of excreted contrast material in the renal collecting systems, usually at about 120 seconds or longer.
Extrarenal (Vicarious) Excretion
In patients with normal renal function, <5% to 10% of injected low-osmolality contrast media is excreted via a nonrenal route. The primary routes of nonrenal excretion are through the biliary tract and the small bowel. In normal circumstances, this excretion is not detectable on plain radiographs, even when a high dose of contrast media is employed. Contrast media may be visible normally in the gallbladder, however, on CT scans obtained 15 to 48 hours after a large dose of contrast media is administered. This visibility is presumed to be related to the high contrast sensitivity of CT and is not a manifestation of renal or hepatic disease.
In patients with depressed renal function, however, excretion of the contrast material via the biliary and small bowel routes is increased and may be visible on plain films. Such excretion has been termed vicarious excretion. The exact mechanism for this phenomenon is not certain, but it is speculated that, in such patients, protein binding of the contrast media occurs and results in increased hepatic excretion. In addition to biliary excretion, there is evidence of direct transmural excretion of contrast media through the small bowel. Such excretion is usually not visible until the contrast media reaches the colon, where water absorption increases the concentration of the contrast media. Direct colon excretion of the contrast media is not thought to occur. There has been a concern that the administration of contrast media to patients with little or no renal function might have adverse hemodynamic effects, and therefore, immediate hemodialysis after contrast administration should be instituted. However, it has been shown that immediate postprocedure dialysis is not necessary and that even functionally anephric patients can be given nonionic contrast media with no discernible adverse effects. The contrast media so administered will eventually be excreted through biliary and small bowel routes and also removed at the time of subsequent dialysis.
CONTRAST MEDIA: PACKAGING
As can be seen, a variety of physical and chemical properties may be used to describe the contrast media in general use in the United States, the most important of which are ionicity and osmolality. With the older, ionic contrast media, the strength of the contrast media was frequently expressed in terms of percent contrast molecule concentration. This number represents the number of grams of the total contrast molecule per 100 mL of water. This designation does not, per se, describe the amount of iodine in solution, but in general, the higher the percent concentration, the more radiopaque the contrast media. Currently, many commonly used contrast media use a numerical designation to denote the amount of iodine in milligrams per milliliter of the contrast media. Thus, Conray 325 (Mallinckrodt Imaging, Hazelwood, MO), an ionic monomer, contains 325 mg of iodine per mL of solution. Isovue 370 (Bracco, Monroe, NJ), a nonionic monomer, contains 375 mg of iodine per mL of solution.
ACUTE ADVERSE REACTIONS TO CONTRAST MEDIA
Reactions to contrast media, although uncommon, continue to constitute a significant hazard to patients despite considerable research into their nature, incidence, and mechanisms. Fortunately, most adverse reactions are mild and self-limited, with symptoms including a metallic taste in the mouth, a sensation of warmth, and, occasionally, a few hives.
Adverse effects of contrast media can be divided into two groups: (1) allergic-like reactions, those which mimic an allergic response to contrast media, and (2) physiologic or chemotoxic effects, those thought to be secondary to a direct toxic effect of the contrast media. Because many of the allergic-like reactions to contrast media mimic those produced by true known allergens (i.e., urticaria or bronchospasm), but are not mediated by immunoglobulins, these reactions are sometimes referred to as “anaphylactoid” or “allergic-like” rather than anaphylactic.
ACUTE ALLERGIC-LIKE REACTIONS
Allergic-like reactions to nonionic contrast material are rare, in one series of more than 80,000 patients reported by Wang et al, occurring in 0.6% of patients injected for CT. Allergic-like reactions can be classified as (1) mild, (2) moderate, or (3) severe, with the vast majority of reactions being mild. Mild reactions are defined as those having only minor effects requiring no therapy. Moderate reactions are those that are transient and not life-threatening but usually requiring therapy. Severe reactions are defined as those that are life-threatening and that require intensive therapy. The more commonly encountered symptoms of these different types of allergic-like reactions are listed in Table 2.1.
Mechanism of Allergic-Like Contrast Reactions
There is no universally accepted mechanism that explains the diverse manifestations of allergic-like contrast reactions. Although an antigen-antibody-mediated mechanism has been suggested by some investigators, evidence indicates that, in the majority of cases, contrast reactions are not true allergic reactions. The fact that some patients react on their first exposure to contrast media (before any sensitization), that reactions are not consistent (upon reexposure), and that most repeat reactions are not progressive militates against the standard immune response theory. In addition, there are only occasional reports of circulating antibodies to contrast material having been identified. Some of these studies have shown, however, that a few patients manifesting anaphylaxis symptoms beyond simple urticaria have IgE-mediated reactions that can be detected through skin testing. Nonetheless, such testing has not been recommended as a routine procedure, as this will not detect the vast majority of patients for whom reactions occur unpredictably.
A variety of immune modulators appear to be involved in at least some contrast reactions. Contrast media can induce histamine release from mast cells and basophils without immunoglobulin mediation, but whether this can occur in sufficient quantities to produce the type of reaction seen with contrast hypersensitivity has been questioned. Activation of the complement system has also been shown to occur after contrast administration, and this mechanism is implicated by some, but whether a cause-and-effect relationship between complement activation and the clinical syndrome of contrast sensitivity exists remains in doubt. Attention has also been directed to the contact system as a cause of reactions to contrast media. This system begins with activation of clotting factor XII (possibly by local disruption of the vascular endothelium as a result of the needle puncture and the introduction of the contrast media) and continues as a cascade involving the activation of kallikrein from prekallikrein and kinins from high molecular weight kininogens.
TABLE 2.1 Symptoms of Contrast Material Reactions
Mild
Physiologic
Dizziness
Headache
Heat sensation
Nausea
Mild vasovagal reaction (resolving quickly and without treatment)
Mild vomiting, retching
Arm pain
Allergic-like
Mild urticaria or edema
Limited cutaneous edema
Nasal congestion
Sneezing/stuffy nose/watery/red eyes
Moderate
Physiologic
Chest pain (angina)
Hypertension
Hypotension and bradycardia (vasovagal) requiring treatment
Protracted nausea or severe vomiting
Allergic-like
Generalized urticaria
Bronchospasm with mild or no hypoxia
Facial edema without dyspnea
Throat tightness or hoarseness without dyspnea
Severe
Physiologic
Arrhythmia
Cardiopulmonary arrest
Hypertensive crisis
Loss of consciousness
Pulmonary edema
Vasovagal reaction resistant to treatment
Seizures
Allergic-like
Bronchospasm resistant to treatment and/or with hypoxia
Loss of consciousness, including cardiopulmonary arrest
Laryngeal edema with stridor and/or hypoxia
Hypotension (systolic blood pressure <70 mm Hg) and tachycardia (rate > 100 bpm)
Pulmonary edema
Sustained cardiac arrhythmia
From ACR Manual on Contrast Media (v. 10.1)
Risk Factors
Allergies and Asthma
A number of risk factors have been identified that place patients at increased risk for having an allergic-like contrast reaction (Table 2.2). A history of a previous reaction to the administration of contrast media is the greatest single predictor of an untoward reaction to a subsequent contrast media injection, increasing the risk of a subsequent reaction by a factor of about five. Fortunately, only a small minority of such patients will have an adverse reaction to a subsequent contrast injection. Thus, a history of prior mild or moderate reaction to contrast media should not be taken as an absolute contraindication to reexamination when a repeated study is based upon sound medical indications. A history of a severe reaction to contrast media, however, is considered a relative contraindication to reexamination in all, but the most urgent cases, due to the concern that should such a patient have another reaction, it could be equally, or even more, severe.
A history of prior exposure to contrast media without difficulty in the past does not confer immunity to a subsequent contrast reaction. Multiple cases have been reported in which patients suffered a contrast reaction after several prior studies that were performed without difficulty, or in which patients have reacted inconsistently to subsequent contrast material injections.
Patients with a history of allergy to food, drugs, and seasonal allergies (i.e., hay fever) or asthma also have an increased chance of having a contrast reaction, but the magnitude of this increased risk varies in the reported series (usually only doubling or tripling the risk of an adverse reaction in comparison to all exposed patients).
Shellfish
Although shellfish and contrast material both contain iodine, there is not believed to be any specific cross-reactivity. Therefore, patients with shellfish allergies are not felt to be at any significantly increased risk of having a contrast reaction, at least when compared to patients with other food or medication allergies. Contact allergy to iodine-containing products is also thought to be unrelated to contrast sensitivity. As such, sensitivity to such iodine-containing products such as povidone-iodine solution (Betadine; The Purdue Frederick Co., Norwalk, CT) should not be considered an absolute contraindication to the administration of iodinated contrast media.
Age
The incidence of mild, moderate, and severe reactions is approximately equal in all age groups. The data do not validate the commonly held notion that reactions are virtually unknown in the pediatric population. In fact, the large multicenter study by Katayama et al., published in 1990, found that there was a higher incidence of reactions in younger patients. However, most contrast reaction deaths occur in patients with significant preexisting cardiac or vascular disease.
Only gold members can continue reading. Log In or Register to continue