and Jurgen J. Fütterer2, 3
(1)
Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Rome, Italy
(2)
Department of Radiology and Nuclear Medicine, Radboudumc, Nijmegen, The Netherlands
(3)
MIRA Institute for Biomedical Technology and Technical Medicine, University of Twente, Enschede, The Netherlands
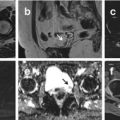
Germ Cell Tumor, Ovarian
Ovarian germ cell neoplasms (OGCNs) may be benign or malignant. These neoplasms comprise approximately 20–25 % of ovarian neoplasms overall and arise primarily in young women aged between 10 and 30.
Germ cell tumors are a histologically heterogeneous group of tumors. The main categories of ovarian germ cell tumor are teratomas (the most common benign OGCNs), immature teratomas, dysgerminomas, endodermal sinus or yolk sac tumors, and mixed germ cell tumors. These conditions are bilateral in 10–12 % of cases, while the majority of other histologies present as unilateral ovarian masses. OGCNs often produce hormones, particularly the beta subunit of human chorionic gonadotropin (hCG), and grow rapidly.
Patients typically present with one or more symptoms: abdominal enlargement (from the mass itself, ascites, or both; in 87 % of patients), abdominal pain (from rupture, hemorrhage, or torsion; in 85 % of patients), precocious puberty, abdominal distention, fever, abnormal vaginal bleeding (presumably from hCG production), and symptoms of pregnancy (from hCG production).
In virtually all cases, surgery is required for definitive histological diagnosis, treatment, and staging (if malignant) of OGCNs.
CT has high sensitivity in the diagnosis of cystic teratomas. Typically, CT images demonstrate fat, fat–fluid level, and calcifications. The presence of most of the above tissues is diagnostic of ovarian cystic teratomas in 98 % of cases. Malignant transformation should be suspected if the size exceeds 10 cm or if a mass with irregular borders is seen. When ruptured, the characteristic hypoattenuating fatty fluid can be found typically below the right hemidiaphragm.
Immature teratoma: On CT images, punctate foci of fat and scattered calcifications are indicative of teratoma. The cystic components contain serous fluid or more rarely sebaceous or adipose material. The imaging appearance is typically of a large, heterogeneous mass with fatty elements, coarse irregular calcifications, and numerous cysts of variable sizes. However, the spectrum of appearances ranges from a predominantly cystic to a predominantly solid mass. Hemorrhage may be present.
Ovarian dysgerminoma: At imaging, it appears predominantly as a solid, multilocular, and well-defined lesion. CT is able to visualize punctate calcifications and areas of attenuation due to necrosis or hemorrhage. After contrast medium administration, the malignancy shows marked enhancement, especially in the fibrovascular enhancing septa, calcification may be present in a speckled pattern.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree