Techniques
- ◼
Fluoroscopy is an imaging modality where continuous x-ray images are obtained to evaluate the body in real time, often with the aid of administered radiopaque contrast material ( Fig. 2.1 ).

Fig. 2.1
Schematic diagram of a fluoroscopic imaging system.
- ◼
Fluoroscopic examinations attempt to answer specific questions, and therefore understanding the indications and limitations of each examination is crucial.
- ◼
Imaging with fluoroscopy is heavily operator controlled, allowing for wide customization and personalization of each study.
Types and indications of fluoroscopic procedures in the abdomen and pelvis include:
| Gastrointestinal Fluoroscopic Procedures | Indications |
| Modified Barium Swallow | Esophageal symptoms, e.g., dysphagia, hiatal hernia, reflux |
| Upper GI study | Stomach evaluation, e.g., gastritis, mass, ulcers |
| Postoperative upper GI leak study | Leak or obstruction following gastric bypass ( Fig. 2.2 ) |
| Small bowel follow through | Small bowel transit time, obstruction, inflammatory bowel disease ( Fig. 2.3 ) |
| Stoma examinations | Presurgical planning |
| Fistulogram | Presurgical planning |
| Enema | Rectal obstruction, presurgical planning, anastomotic integrity |
| Enteroclysis | Direct contrast administration through NG tube to evaluate small bowel |
| Genitourinary Fluoroscopic Procedures | |
| Cystogram | Bladder perforation, bladder capacity prerenal transplant |
| Voiding cystourethrography | Vesicoureteral reflux |
| Retrograde urethrography | Anterior urethral injury, stricture |
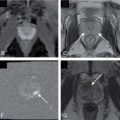
| Hysterosalpingogram | Patency of fallopian tubes, uterine abnormalities ( Fig. 2.4 ) |
| Interventional Procedures | |
| Placement of vascular catheters and stents | |
| Placement of drainage catheters | |
| Urological procedures, e.g., retrograde pyelography, percutaneous nephrostomies, and suprapubic cystotomies | |
| Hydrostatic reduction of intussusceptions and sigmoid volvulus |



Fluoroscopic contrast agents
- ◼
Contrast agents are compounds that enable improved visualization of internal luminal structures, spaces, and tracts, and allow for controlled real time evaluation of targeted organs.
- ◼
Fluoroscopic contrast agents are divided into two types: positive and negative contrast. Positive contrast materials, such as barium and iodine compounds, absorb x-rays more strongly than surrounding tissues and appear radiopaque. Conversely, negative contrast materials, such as air or CO 2 , absorb x-rays less strongly and are radiolucent.
Barium sulfate
- ◼
Barium sulfate is an element compound that is mixed with water and either ingested or instilled into the gastrointestinal tract. Differing concentrations of barium sulfate suspensions are used to evaluate the wall lining, size, shape, contour and patency of the hollow viscus.
- ◼
Barium is an inert element; allergic reactions are exceedingly rare. It is the contrast agent of choice when evaluating for aspiration because barium can be coughed out without major issue. Conversely, barium is contraindicated in the evaluation of possible bowel perforation, as barium within the abdominal cavity can cause peritonitis.
- ◼
Side effects of barium include: bloating, constipation, cramping, nausea or vomiting.
Water-soluble agents
- ◼
Water-soluble contrast agents can be divided into ionic or nonionic agents or, depending on the osmolarity, as high- and low-osmolar agents. Nonionic agents have lower osmolarity and demonstrate fewer side effects. Water-soluble agents are used when barium is contraindicated, specifically in the evaluation of perforation.
- ◼
Water-soluble agents have multiple disadvantages. These agents are less radiodense than barium and result in poorer opacification of the gastrointestinal tract. In addition, the high osmolar content of these agents causes rapid dilution of these agents as it travels in the distal small bowel.
- ◼
In patients with suspected aspiration, water-soluble agents are contraindicated. Aspiration or these agents can lead to pneumonitis and severe pulmonary edema because of their high osmolarity.
- ◼
Gastrografin (diatrizoate meglumine and diatrizoate sodium) is a noniodine based water-soluble contrast agent that can be used in patients with iodinated contrast allergy.
Equipment factors
- ◼
Source-to-image distance (SID).
- ◼
Fluoroscopic kilovoltage peak (kVp).
- ◼
Fluoroscopic milliampere (mA).
- ◼
Focal spot.
- ◼
Field of view.
- ◼
Grid use.
- ◼
Fluoroscopic acquisition mode.
- ◼
Dose rate selection.
- ◼
Video frame rate.
Pearls for maximizing image quality and minimizing radiation exposure
- ◼
Collimate image to match axis of organ being evaluated.
- ◼
Keep image intensifier as close to patient as possible.
- ◼
Use rapid sequence option only to document motion abnormalities or to catch a rapidly changing segment that can only be evaluated with a single shot.
- ◼
A fluoroscopic store option is available for an image that one wishes to record.
Protocols
Barium swallow (esophagram)
- ◼
Fluoroscopy is the main radiology modality for evaluation of the esophagus. Fluoroscopy is uniquely suited for the evaluation of dynamic oropharyngeal function, esophageal morphology, motility, mucosa, gastroesophageal (GE) junction, and reflux.
- ◼
Evaluation of the esophagus can be performed either with single-contrast or double-contrast technique. Single-contrast examination is usually performed with ingestion of oral barium. A double-contrast technique involves first ingesting an effervescent agent to allow for gaseous distention of the esophagus before barium administration.
Anatomy
- ◼
The esophagus is approximately 20 to 35 cm long and divided into the cervical, thoracic and abdominal esophagus.
- ◼
The esophagus begins at the cricopharyngeus (upper esophageal sphincter) and ends at the lower esophageal sphincter (or ampulla/vestibule).
Technique
Patient should be nothing-by-mouth (NPO) for the examination.
- ◼
Scout with collimation for foreign body, metal, or in the evaluation of fistula or leak.
- ◼
Effervescent crystals for double-contrast examination.
- ◼
Dynamic evaluation of pharynx with lateral and anteroposterior (AP) projection for aspiration.
- ◼
Upright left posterior oblique (LPO) for distal esophagus.
- ◼
Horizontal right anterior oblique (RAO) for esophageal motility, mucosal abnormality, GE junction.
- ◼
Supine, slowly rolling toward the right (Schatzki maneuver) with provocative maneuvers for reflux (cough, Valsalva). Water siphon test can be considered.
- ◼
Brief examination of the stomach and proximal bowel for gross abnormalities.
- ◼
Upright swallow of barium tablet for functional obstruction.
Normal esophageal impressions
- ◼
Cervical impression because of the cricoid cartilage at C5–C6.
- ◼
Thoracic impression because of the aortic arch at T4–T5.
- ◼
Abdominal impression because of the diaphragm at T10–T11.
Abnormalities on esophagram
Esophageal dysmotility
Fluoroscopy is uniquely suited for the evaluation of motility abnormalities, which include:
- ◼
Achalasia: failure of the lower esophageal sphincter to relax, with decreased peristalsis. “Birdbeak” appearance with smooth tapering.
- ◼
Pseudoachalasia: irregular narrowing of the lower esophageal sphincter because of infiltrative tumor with irregular lobulations.
- ◼
Diffuse esophageal spasm: intermittent, uncoordinated contractions, which cause a “corkscrew” appearance that can lead to chest pain or dysphagia.
- ◼
Scleroderma: absent peristalsis of the smooth muscle leading to a dilated distal esophagus.
Diverticula
- ◼
Zenker’s: most common, arises at Killian’s dehiscence near the pharyngoesophageal junction; posterior.
- ◼
Killian-Jameson: just inferior to Zenker’s; lateral ( Fig. 2.5 ).