Anatomy, embryology, pathophysiology
Embryology
Splenogenesis initiates in the fifth week of embryological life. The dorsal mesogastrium anchors the stomach posteriorly; it is within the two leaves of this mesogastrium that the spleen forms from mesenchymal cells. Asymmetric stomach growth results in rotation of the spleen from the midline to its final position in the left upper quadrant. The mesogastric connection becomes the gastrosplenic ligament. Medial to the gastrosplenic ligament is the lesser omental bursa and the infolding lateral surface of the ligament fuses to the left kidney resulting in the splenorenal ligament. Normal fetal lobulations of the spleen are the result of fusing mesodermal buds. Incomplete fusion can result in deep clefts or complete separation as the dorsal mesogastrium fuses about the spleen, giving accessory spleens.
- ◼
Accessory spleens can be seen in the splenic hilum, along the splenic vasculature, within the gastrosplenic or splenorenal ligaments, in the pancreatic tail, in the gastric wall, and rarely in the scrotum. Accessory spleens should follow the imaging characteristics of the spleen on all imaging modalities.
- ◼
Wandering spleen results from malformation, laxity, or disruption of the gastrosplenic or splenorenal ligaments; it can be congenital or acquired.
- ◼
Predisposed to torsion and trauma. Ectopia is the predominant imaging finding.
- ◼
“Whirl” sign of splenic vessels and pancreatic tail can be seen in torsion. Resultant infarction is hypodense to the liver on computed tomography (CT). With preserved collateral flow, the capsule remains hyperdense, giving the “rim” sign.
- ◼
Treatment for symptomatic patients is splenopexy or splenectomy if infarcted.
- ◼
- ◼
Polysplenia/asplenia occur in the setting of a visceral heterotaxia syndrome.
- ◼
Polysplenia is seen in left isomerism with female predominance. A variable number of spleens and accessory spleens are seen in the upper abdominal quadrant containing the stomach (right or left).
- ◼
Asplenia is seen in right isomerism with male predominance.
- ◼
Both syndromes are associated with complex congenital heart disease, midline liver and gallbladder, truncated pancreas, bowel malrotation, and caval abnormalities. Left isomerism features bilobed lungs with hyparterial bronchi whereas right isomerism has trilobed lungs with eparterial bronchi.
- ◼
Techniques
- ◼
Ultrasound (US) can be used for posttraumatic screening to assess for hemoperitoneum, which may suggest splenic injury.
- ◼
99m Tc-sulfur colloid scintigraphy will show reticuloendothelial uptake and photopenia where normal splenic parenchyma is absent. Once routine, this study is primarily used to locate/confirm ectopic splenic tissue.
- ◼
CT: Axial arterial and portal venous phase CT are used to characterize masses, vascular abnormalities, and traumatic injuries. The spleen demonstrates a normal striated enhancement pattern on arterial phase imaging with homogeneous enhancement on portal venous phase.
- ◼
Magnetic resonance (MR): T1 and T2 weighted imaging with gadolinium contrast media can be used to characterize splenic lesions. The spleen normally demonstrates diffusion restriction.
- ◼
Fluorodeoxyglucose–positron emission tomography (FDG-PET): Not typically used for focal evaluation of the spleen. Most commonly used to assess for intrasplenic and extrasplenic lymphoma.
- ◼
Radiography can demonstrate gross abnormalities on splenic size (e.g., splenomegaly or autoinfarction) and the presence of calcification, but is not generally used for splenic evaluation and will not be discussed further.
Protocols
- ◼
Portal venous phase CT is used for routine evaluation. Assessment of vascular abnormalities, trauma, and masses should be done with arterial and portal venous phases. Coronal reconstructions should be viewed to best evaluate organ size.
- ◼
Magnetic resonance imaging (MRI): T1-weighted and T2-weighted sequences in the axial and coronal planes with postcontrast T1-weighted arterial phase and venous phases sequences enable characterization of most splenic processes. When hemosiderin deposition is suspected, a T2* sequence can be added.
- ◼
Tc99m scintigraphy is done by labelling either sulfur colloid or red blood cells, which are then heat damaged.
Specific disease processes
Focal splenic lesions
- ◼
Splenic cysts:
- ◼
Primary cysts are lined with epithelium and are developmental in origin. Secondary cysts lack epithelial lining and more most likely the result of trauma and less commonly seen after infarction, infection, and pancreatitis ( Fig. 20.1 ).
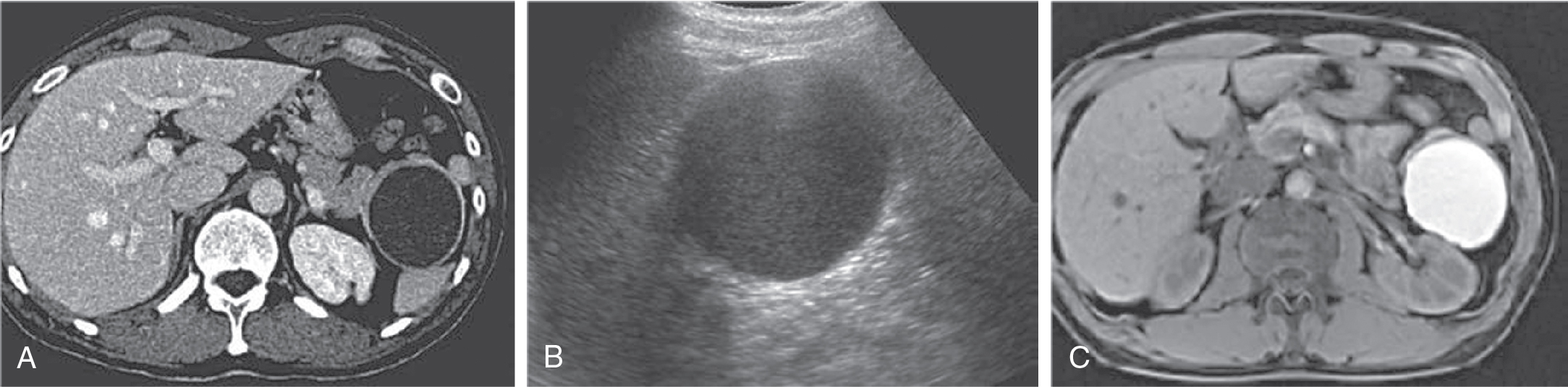
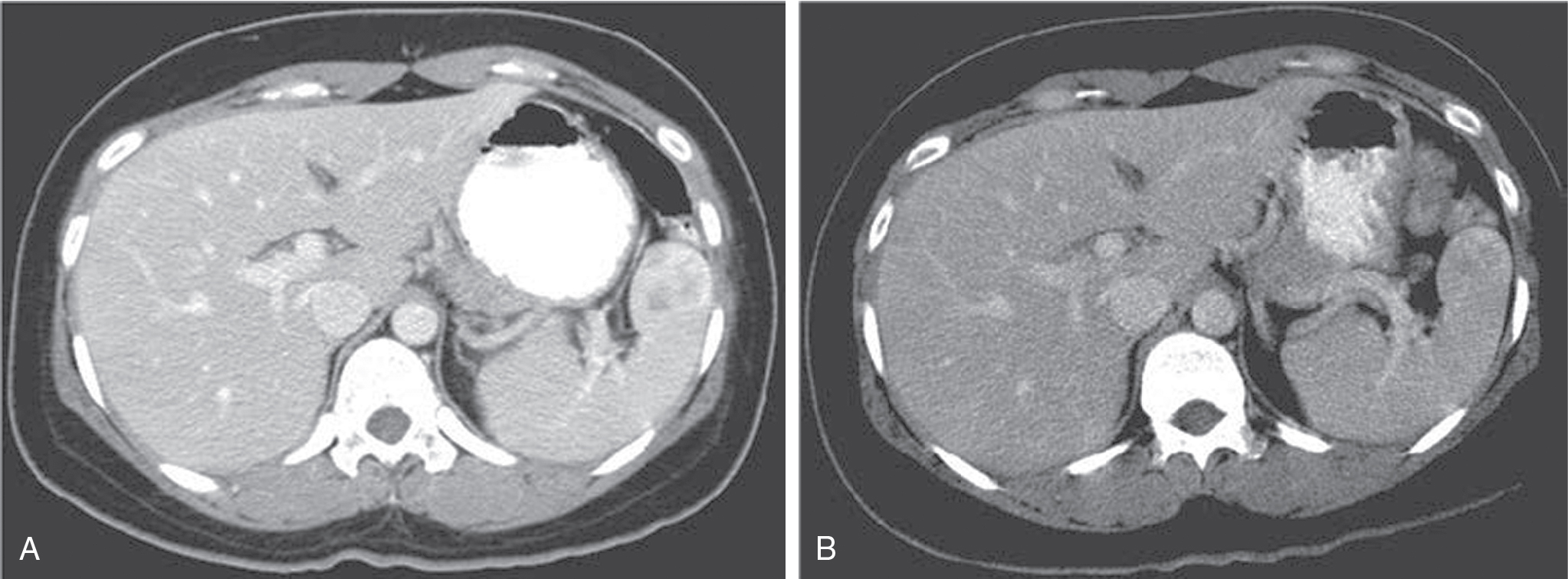
Fig. 20.1
Splenic epidermoid cyst as seen on (A) computed tomography, (B) ultrasound, and (C) fat-suppressed T1-weighted magnetic resonance imaging.
- ◼
Typically asymptomatic and an incidental finding, including in accessory splenic tissue. Can be symptomatic because of large size, hemorrhage, rupture, or infection. History will drive diagnosis and symptoms will drive treatment, including surgery.
- ◼
Imaging appearance is typical of cysts on all modalities, with variable internal appearance on T1-weighted MRI and US determined by cyst contents (e.g., protein, blood products, etc.). Nonspecific photopenia is seen on scintigraphy. Calcification is more common in secondary cysts ( Fig. 20.2 ).
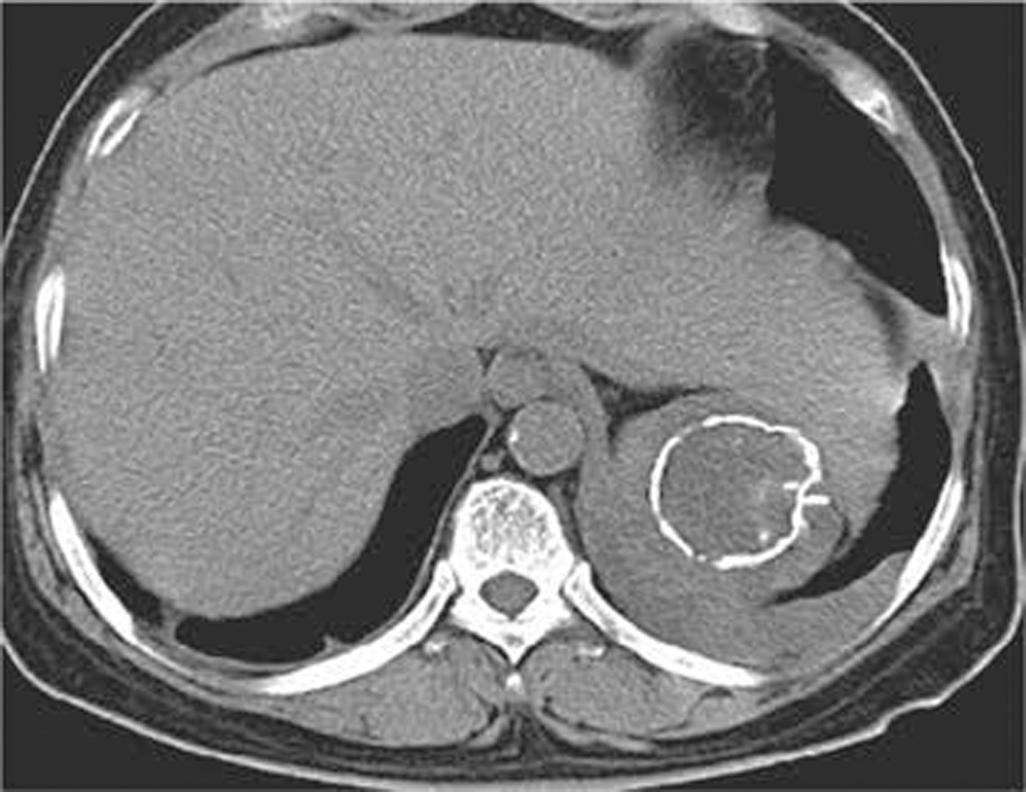
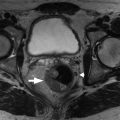
Fig. 20.2
Calcified splenic pseudocyst on computed tomography.
- ◼
Benign splenic tumors
- ◼
Hemangioma:
- ◼
Most common benign tumor and usually asymptomatic. Large size or blood product sequestration may prompt symptomatic presentation and determine treatment.
- ◼
Hemangiomas are iso- to hypodense on unenhanced CT, iso- to hypointense on unenhanced T1-weighted MRI, and hyperintense on T2-weighted MRI. Punctate and/or curvilinear calcifications are variably present.
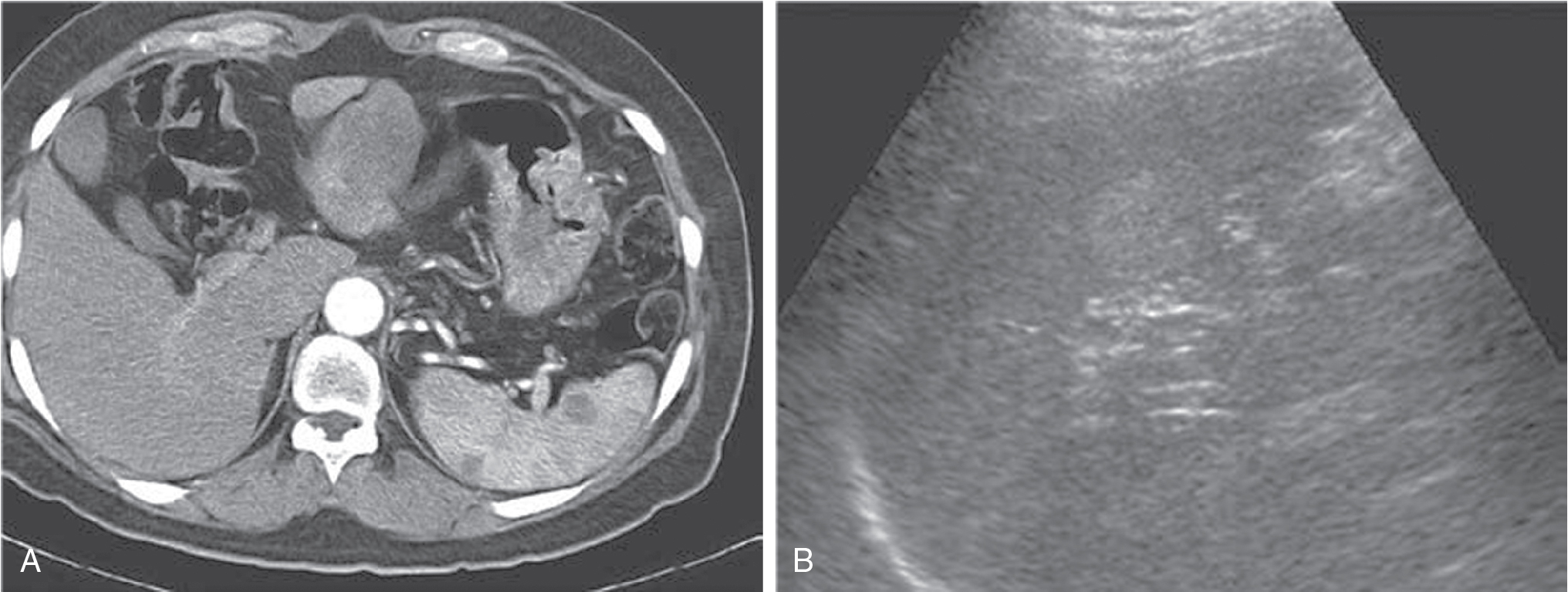
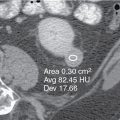
Fig. 20.3
Splenic hemangiomas as seen on (A) arterial phase contrast enhanced computed tomography and (B) ultrasound.
- ◼
Variable enhancement pattern on CT and MRI, although typically hypoenhancing relative to normal venous phase splenic parenchyma ( Fig. 20.3 ). Hyperenhancement can be seen on arterial phase images.
- ◼
- ◼
Hamartoma:
- ◼
Asymptomatic hypervascular lesion usually occurs in the mid-organ along the convex (outer) surface and can be seen in hamartoma syndromes. This is a well-defined solid lesion with mass effect on adjacent normal spleen.
- ◼
Can be isodense on pre- and postcontrast CT with the outer surface contour abnormality being the only CT evidence ( Fig. 20.4 ).
- ◼