Phenotypic finding
Cardiac features
Diseases to consider
Sensorineural deafness
HCM
Mitochondrial diseases
Anderson–Fabry disease
LEOPARD syndrome
DCM
Epicardin mutation
Mitochondrial diseases
Muscle weakness
HCM
Mitochondrial diseases
Glycogenosis
DCM
Dystrophinopathies
Sarcoglycanopathies
Laminopathies
Myotonic dystrophy
Desminopathies
RCM
Desminopathies
Learning difficulties, mental retardation
HCM
Mitochondrial diseases
Noonan Syndrome
Danon disease
DCM
Dystrophinopathies
Mitochondrial diseases
Myotonic dystrophy
FKTN mutations
RCM
Noonan syndrome
Myotonia (involuntary muscle contraction with delayed relaxation)
Myotonic dystrophy (type 1 and type 2)
Paraesthesia/sensory abnormalities/neuropathic pain
HCM
Amyloidosis
Anderson–Fabry disease
RCM
Amyloidosis
Table 2.2
Examples of skin/eyes signs that should raise suspicion of specific cardiac features
Phenotypic finding | Cardiac features | Disease to be considered |
|---|---|---|
Visual impairment | HCM | TTR-related amyloidosis (vitreous opacities, cotton wool type) |
Danon disease (retinitis pigmentosa) | ||
Anderson–Fabry disease (cataracts, corneal opacities) | ||
DCM | CRYAB (polar cataract) type 2 myotonic dystrophy (subcapsular cataract) | |
Carpal tunnel syndrome (bilateral) | HCM | TTR-related amyloidosis |
RCM | Amyloidosis | |
Lentigines/café au lait spots | HCM | LEOPARD syndrome |
Angiokeratoma hypohidrosis | HCM | Anderson–Fabry disease |
Palmoplantar keratoderma, woolly hair | ARVC | Naxos and Carvajal syndromes |
CMP may also be a feature of rare congenital dysmorphic syndromes that are diagnosed during infancy and childhood [31]. A detailed description of these disorders is outside of the aim of this chapter. It is evident that CMP are a common feature of multisystem diseases. The mechanisms of multiorgan involvement are heterogeneous, and a complete evaluation includes researching red flags, such as the following [32, 33]:
Get Clinical Tree app for offline access

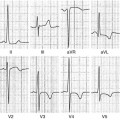
Electrocardiogram abnormalities (Table 2.3)
Table 2.3
Laboratory findings that should raise the suspicion of specific cardiac features
High serum creatine kinase (CK)
HCM
Mitochondrial diseases
Glycogenosis
Danon disease
DCM
Dystrophinopathies
Sarcoglycanopathies
Zaspopathies (LDB3 gene)
Laminopathies
Myotonic dystrophy
FKTN mutations
RCM
Desminopathies
Myofibrillar myopathies
Proteinuria with/without low glomerular filtration rate
HCM
Anderson–Fabry disease
RCM
Amyloidosis
High transaminase
HCM
Mitochondrial diseases
Glycogenosis
Danon disease
High transferrin saturation/hyperferritinemia
DCM
Hemochromatosis
RCM
Lactic acidosis
HCM
Mitochondrial diseases
DCM
Myoglobinuria
HCM
Mitochondrial diseases
DCM
Leukocytopenia
HCM
Mitochondrial diseases (TAZ gene/Barth syndrome)
DCM
Laboratory tests (Table 2.4)
Table 2.4
Examples of electrocardiographic (ECG) abnormalities that should raise the suspicion of specific diagnoses grouped according to the main cardiac features
Phenotypic finding
Cardiac features
Diseases to be considered
Short PR/pre-excitation (WPW like)
HCM
Glycogenosis
Danon
PRKAG2
Anderson–Fabry
Mitochondrial disease
AV block
HCM
Amyloidosis
Danon disease
DCM
Laminopathy
Emery Dreifuss
Sarcoidosis
Desminopathy
RCM
Desmin-related cardiomyopathy
Amyloidosis
Extreme LV hypertrophy (Sokolow criteria)
HCM
Danon disease
Pompe disease
Low QRS voltage
HCM
Amyloidosis
Low P wave amplitude atrial standstill
DCM
Emery Dreifuss
Q waves in posterolateral leads
DCM
Dystrophin-related cardiomyopathy
Limb-girdle muscular dystrophy
Sarcoidosis
Inverted T waves in inferolateral leads
ARVC
ARVC with biventricular involvement
Epsilon waves in inferolateral leads
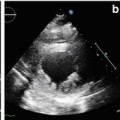
Echocardiography/cardiac magnetic resonance: hypertrophy pattern, pericardial effusion, valve thickening, bulging, sacculations, sparkling myocardium texture, late gadolinium enhancement (LGE) (Table 2.5). Some typical features are described, such as LGE localized to the inferolateral wall in patients with Anderson–Fabry disease or dystrophinopathies and to the circumferential subendocardial wall in cardiac amyloidosis. The echocardiogram remains the first-line imaging tool in patients with suspected CMP. It has a central role in defining the morphological and functional phenotype and in guiding treatment decisions. As with all imaging modalities, echocardiography rarely suggests a specific etiology, but it can be helpful in the context of a number of features in directing further investigation.
Table 2.5Related posts:
 Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Hypertrophic Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Arrhythmogenic Right Ventricular Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
Arrhythmogenic Right Ventricular Cardiomyopathy: Usefulness of Imaging in Prognostic Stratification and Choice of Treatment
 Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
Arrhythmogenic Right Ventricular Cardiomyopathy: Clinical Assessment and Differential Diagnosis
 Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
Advanced Echocardiographic Technologies in Dilated Cardiomyopathy
 Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
Infiltrative/Storage Cardiomyopathies: Clinical Assessment and Imaging in Diagnosis and Patient Management
 Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management
Restrictive Cardiomyopathy: Clinical Assessment and Imaging in Diagnosis and Patient Management

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

