Germ and Stromal Cell Tumors of the Gonads and Extragonadal Germ Cell Tumors
Germ and Stromal Cell Tumors of the Gonads and Extragonadal Germ Cell Tumors
Christian Carrie
Edward C. Halperin
Gonadal or extragonadal germ cell tumors (GCTs) represent less than 2% of pediatric malignant tumors. They have three important features:
The origin is related to abnormal migration of primordial germ cells and tumor can occur along this migration path.
Serum tumor markers allow diagnostic and treatment evaluation.
The cure rate is high if the clinician respects treatment guidelines.
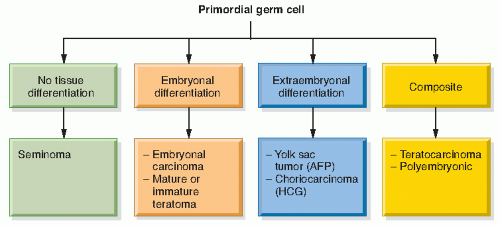
GCTs result from malignant transformation of a primordial germ cell (Fig. 15.1)
In the human embryo the primordial germ cells are found in the vicinity of the allantoic stalk. From this position the germ cells migrate into the adjoining mesenchyme at 4-5 weeks of gestation. The cells then assume positions in the germinal ridges and migrate along these structures.
GCTs may occur in the ovary, testes, sacrococcygeal region, vagina, retroperitoneum, pelvis, omentum, and mediastinal areas. Extragonadal and testicular sites predominate in children younger than 3 years old. Gonadal sites are most common during and after puberty (1). The main histologic types are germinoma, embryonal carcinoma, yolk sac tumor (also known as endodermal sinus tumor or Teilum tumor), malignant mixed GCTs, and malignant teratomas (sometimes called immature teratomas) (Table 15.1) (2, 3, 4, 5). Endodermal sinus tumor typically shows microcytic areas, Shiller-Duval bodies, and periodic acid-Schiff-positive extracellular hyaline droplets. The tumor is often positive, on immunohistochemistry, for α-fetoprotein (AFP) and cytokeratin (6). Structural abnormalities of chromosome 1 are frequent (1).
Figure 15.1 Classification of germ cell tumors.
Teratomas (from Greek teratos, “monster,” and onkoma, “swelling”) are the most common pediatric GCTs. Malignant teratomas may develop anywhere along the pathway of germinal tissue migration. By definition, teratomas are composed of tissues derived from two or three germinal layers (tridermal ancestry): ectoderm, mesoderm, and endoderm. Malignant teratomas are so named because of foci of endodermal sinus tumor, embryonal carcinoma, germinoma, or choriocarcinoma. There may also be foci of neuroblastoma, nephroblastoma, or hepatoblastoma. In general, frank malignancy is identified in about 20% of teratomas (5). The distinction must be made between immature teratomas with distinct malignant elements, which warrant aggressive adjuvant therapy, and immature teratomas with primitive neuroepithelium, which can be cured with surgery alone. Immature teratomas are graded by the system of Norris, which also predicts relapse (Table 15.2).
GENERAL ASPECTS OF CLINICAL PRESENTATION, STAGING, AND WORKUP
There is a bimodal age distribution for GCTs, with a peak in children younger than 3 years old and a second peak in children older than 12 years. The male:female ratio is 2:1 (9). Girls predominate in the patient population during the first 3 years of life because of a female predominance in sacrococcygeal tumors (SCTs). There is an association with intersex disorders (1,10,11). The association between undescended testes and the development of testicular cancer has been established.
Table 15.1 Biological Characteristics of Pediatric Germ Cell Tumors
Type
Grade
AFP
HCG
Chemotherapy Response
Radiotherapy Response
Dysgerminoma
Malignant
–
+/−
+ + +
+ + +
Embryonal carcinoma
Malignant
–
–
+ + +
+
Yolk sac tumor
Malignant
+ + +
–
+ + +
+
Choriocarcinoma
Malignant
–
+ + +
+ + +
+
Mature and immature teratomas
Benign to potentially malignant
+/−
–
+
+
AFP, α-fetoprotein; HCG, human chorionic gonadotropin.
Derived from Gobel U, Schneider DT, Calaminus G, et al. Germ-cell tumors in childhood and adolescence. Ann Oncol. 2000;11:263-271.
The staging workup should include assays for AFP and human chorionic gonadotropin (HCG). AFP is elevated in almost all cases of endodermal sinus tumor and in many other patients with GCTs (12,13). Successful treatment, whether by surgery, chemotherapy, or radiotherapy, is regularly associated with AFP decline consistent with its half life of 5 days in infants 2 months or younger, 33 days in 2- to 4-month-olds, and 5 days in children 8 months or older (1,13,14). AFP falling too slowly, failing to normalize after treatment, or rising generally signifies inadequate tumor response and precedes clinical or radiographic evidence of treatment failure. HCG activity is present in some tumors, particularly choriocarcinoma. The half time of β-HCG is 24-36 hours.
Diagnostic imaging of the pelvis and presacral space is best performed with computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (5). The role of a PET scan is not well established, probably not necessary for nonseminomatous tumor and more useful to identify viable tumor in case of residual lesion after chemotherapy (15). CT is useful to assess the presence of pathologic retroperitoneal lymph nodes and extension of tumor into bone. Imaging may show GCTs to be cystic, solid, or a combination of both. Sacrococcygeal and ovarian lesions that are predominantly cystic are less likely to be malignant, whereas solid lesions are more likely to be malignant. However, the correlation is far from perfect. This is particularly important because it argues strongly against using the term solid teratoma as the equivalent of malignant or immature teratoma (4,5,16,17).
Table 15.2 Grading of Immature Teratomas
Grade
Description
Approximate Relapse Rate (%)
0
Mature
10
I
Immaturity with PE limited to one lower-magnification field (×40) per slide
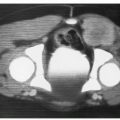
Of primary ovarian tumors of childhood, about 71% are GCTs, 17% epithelial, and 12% sex cord stromal tumors (1,16,18). The histologic distribution is approximately: mature teratoma, 47%; immature teratoma, 12%; dysgerminoma, 5%; yolk sac tumor (endodermal sinus), 10%; mixed GCTs, 0-24%; and choriocarcinoma, <1% (1,7,19) (Fig. 15.2).
The risk of germ cell malignancy in girls more than 3 years old is 20%. All pediatric ovarian tumors must be considered as malignant. In the series by Germa et al. (19), 46% of girls presented with pain. In the POG/CCG intergroup study 11% of girls present with an acute abdomen due to rupture or torsion (20). The long infundibular pedicle in the child explains this risk (12,19). Other presenting signs and symptoms included an asymptomatic palpable mass (19%), abdominal distention (36%), and, less commonly, menstrual irregularities, malaise, nausea, vomiting, or vaginal bleeding (9,19,21, 22, 23, 24, 25, 26, 27, 28, 29, 30). The stromal Sertoli-Leydig cell tumors may present with defeminization or virilization. Ovarian dysgerminomas are rarely hormonally active or productive of tumor markers. If a patient with an ovarian dysgerminoma is found to have an elevated AFP or signs of hormonal imbalance, there should be a meticulous search of the pathology specimen for elements of other tumor. Preoperative assessment is crucial for the postoperative management. Sample AFP, HCG, and β-HCG must be obtained in all solid ovarian tumors.
Figure 15.2 Ovarian dysgerminoma.
Table 15.3 Children’s Oncology Group Surgical Guidelines for Ovarian Germ Cell Tumor in Pediatric Patients
1
Ascites for cytology or peritoneal washing if no ascites present
2
Inspect omentum, resect only if abnormal
3
Inspect and palpate iliac and para-aortocaval nodes; perform biopsy only if abnormal
4
Inspect and palpate controlateral ovary; perform biopsy only if abnormal
5
No violation of tumor capsule in situ for resectable tumors
6
Primary resection for localized tumors; perform biopsy only if resection would require sacrifice of other organs and plan for postchemotherapy resection
From Billmire DF. Germ cell tumors. Surg Clin North Am. 2006;86:489-503, xi, with permission.
Both primary and second-look surgeries are used to treat ovarian GCT. The initial surgical procedure should remove as much tumor as possible with a reasonable possibility of retention of fertility. At the time of laparotomy, the entire peritoneal surface should be examined for the presence of metastasis. Particular attention should be paid to the surfaces of the liver and to the inferior surface of the diaphragm (12). The involved ovary should be removed. Dysgerminoma has a 5-10% incidence of bilaterality (18). For childhood ovarian GCT other than dysgerminoma, the probability of bilateral involvement ranges from 0% to 14% (23). Therefore, the contralateral ovary should be biopsied and, if there is no evidence of malignancy, preserved (29). Palpation and biopsy of all suspicious lymph nodes in the pelvic and para-aortic regions should be done. Peritoneal biopsies and washings (or collection of ascites) for cytology are important to complete the surgical staging (30). When front-line definitive surgery is not possible or appropriate, chemotherapy can be given followed by second-look surgery (31).
Table 15.4 Children’s Oncology Group Staging for Pediatric Ovarian Germ Cell Tumors
Stage
Extent of Disease
I
Limited to ovaries, with no clinical, radiographic, or histologic evidence of disease beyond the ovaries; no malignant cells in ascites or peritoneal washings; omentum grossly normal by visual inspection or pathologically normal if removed; tumor markers normal after appropriate half-life decline (α-fetoprotein = 5 days; β-human chorionic gonadotropin = 16 hours). IA, tumor limited to one ovary; IB, tumor limited to both ovaries
II
Microscopic residual; tumor markers inappropriately elevated; preoperative or intraoperative rupture
III
Retroperitoneal lymph node involvement or metastatic nodule; gross residual or biopsy only; contiguous visceral involvement
IV
Distant metastases, including liver
In the POG study, positive ascetic cytology was found among 100 girls despite negative random biopsy samples. Due to this finding the Children’s Oncology Group (COG) published new guidelines including peritoneal washing (Tables 15.3 and 15.4).
Ovarian GCTs are lethal malignancies that can kill by early metastasis and rapid invasion of abdominal and pelvic structures. The prognosis of girls with these tumors was poor when they were treated with surgery only or surgery in combination with either radiotherapy or single-agent chemotherapy, except in some cases of dysgerminoma (16). An increasing body of evidence indicates that postoperative chemotherapy has increased the probability of survival (1,4,13,16,19,7, 21,22,26, 27, 28, 29). Active drugs include cisplatin (P), carboplatin (J), vinblastine (V), bleomycin (B), adriamycin (Ad), actinomycin (A), cyclophosphamide (C), etoposide (E), methotrexate (M), and vincristine (O) (9,32, 33, 34). Combinations used include VAC, POMB-ACE-PAV, PVB-ACAd, and PEB (5,10,16). PEB or PVB are most commonly used (7,35,36). A six-drug regimen (VAC, JEB or PEB) or JEB therapy both have achieved 5-year survival rates as high as 90% for all stages (37,38).
Only gold members can continue reading. Log In or Register to continue