Chapter 9 Glaucoma
Introduction
The diagnosis of open-angle glaucoma is most commonly made with a combination of intraocular pressure (IOP) measurement, central corneal thickness (CCT) measurement by pachymetry, automated visual field testing (Humphrey Visual Field Analyzer), and optic disc evaluation. Slit lamp examination, while usually normal in primary open-angle glaucoma and normal tension glaucoma, can provide evidence of other open-angle glaucoma mechanisms including pigmentary dispersion, pseudoexfoliation, uveitis, and remote ocular trauma. While slit lamp examination of the anterior segment may provide clues to angle closure,1 gonioscopy is essential for the proper diagnosis and management of the angle-closure glaucoma mechanisms.2 Indentation gonioscopy can help distinguish between appositional angle closure and permanent synechial angle closure.3
A-scan ultrasonography in the glaucoma patient may provide axial length measurements that are longer than normal, indicating myopia. Myopia is more commonly seen in patients with primary open-angle glaucoma and pigmentary glaucoma. Hyperopic patients, with shorter than average axial length, are more likely to have narrow anatomical angles and frank acute, sub-acute or chronic angle-closure glaucoma.4
Preoperative A-scan ultrasonography is essential for intraocular lens implant determination for cataract surgery (Chapter 7). In the presurgical glaucoma patient, A-scan ultrasonography can alert the clinician to longer ocular axial length, a risk factor for inadvertent ocular penetration during retrobulbar anesthetic administration (Chapter 18). Nanophthalmos, typically diagnosed in patients with an ocular axial length less than 21.0 mm, is a risk factor for uveal effusion after routine cataract surgery and for flat anterior chamber and aqueous misdirection after glaucoma filtering surgery.
Anterior chamber angle evaluation
Ultrasound biomicroscopy (UBM) provides excellent, high-resolution images of the ocular anterior segment.5 It can assess conjunctival lesions, corneal disorders and measure the narrowness of the angle and assess the ciliary body. Its high frequency makes it excellent for anterior segment evaluation, but not for posterior segment evaluation because of poor posterior penetration of the high-frequency ultrasound (Chapter 4). Lower frequency B-scan ultrasonography is preferred for posterior segment evaluation in glaucoma patients. UBM requires a highly skilled technician, a supine patient and a water-bath coupling probe on the patient’s eye.
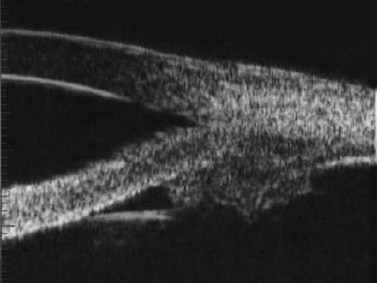
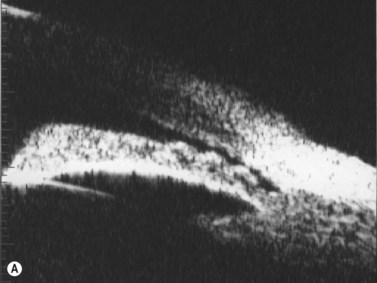
In the normal eye, the UBM will show the cornea and a clear, deep anterior chamber. Just behind that is the flat, undilated iris. Details of the iris stroma and the posterior iris pigment layer are discernable. The central anterior lens capsule surface can be seen just behind the pupil and central iris. More peripherally behind the iris, the ciliary processes, and sometimes zonules, can be seen (Figure 9.1).
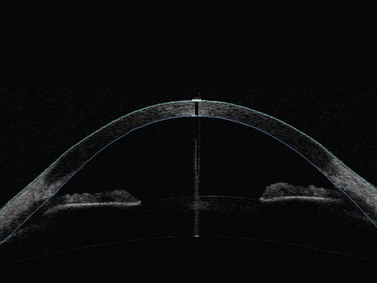
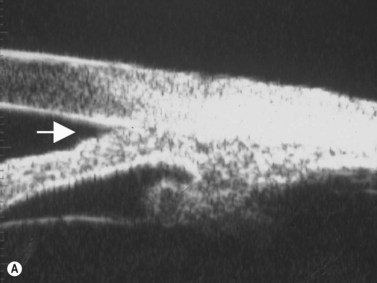
Anterior segment optical coherence tomography (OCT) provides images of the angle structures similar to anterior segment UBM (Figure 9.2).6 It has the advantage of being a non-contact procedure and requires less technical skill than UBM.7,8 Very high frequency digital UBM offers some of the advantages of the anterior segment OCT (Chapter 6).
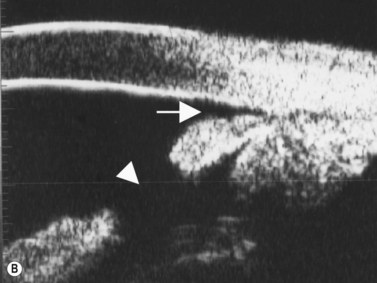
In eyes with a normal and open angle, the iris has a flat approach from the pupil peripherally to the scleral spur. In eyes with a narrow angle, the iris has an anterior convexity and the UBM will show both if the angle is narrowed and by how much (Figure 9.3). In eyes with greater angle narrowing, the UBM will show the peripheral iris touching the scleral spur and the trabecular meshwork region of the angle. This is a dynamic process with the angle opening tending to increase in bright illumination and decrease with angle narrowing in dim illumination.

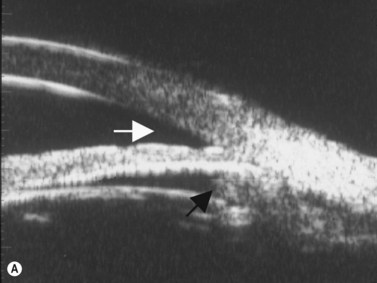
Primary angle-closure glaucoma may present as an acute attack, as intermittent episodes of subacute angle closure, or most commonly, as chronic progressive angle closure, which early on may be asymptomatic. The first two present often with dramatic symptoms of blurred vision, haloes, ocular pain, headache and nausea and vomiting. Shallow anterior chamber, corneal edema, ocular injection, glaucomflecken, and iris atrophy may be seen on slit lamp examination. While glaucoma medical management can reduce intraocular pressure and reduce pain, early laser peripheral iridotomy (LPI) is the treatment of choice for the primary and many secondary angle-closure glaucoma mechanisms. After a successful laser PI, the peripheral iris moves more posteriorly and the anterior chamber deepens. A post-procedural UBM should show a more open angle with less anterior iris convexity. However, peripheral anterior synechiae, adhesions of the iris to the trabecular meshwork and cornea, will persist. The UBM may also show the patency of the LPI (Figure 9.4).
Reproduced with permission from: Rockwood EJ, Sharma S, Hayden BC, Singh AD. Glaucoma. Ultrasound Clin 2008; 3(2):207–215.4
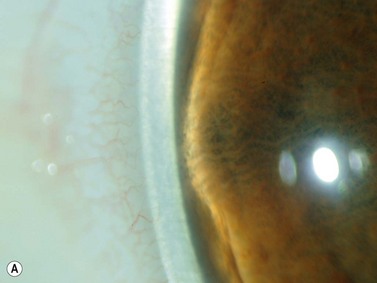
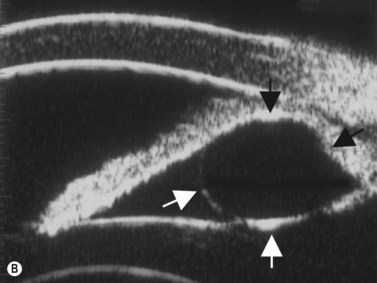
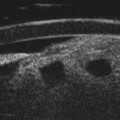
Plateau iris configuration may be seen during gonioscopy. The approach of the iris from the peripupillary region to the peripheral iris may appear relatively flat. However, as the iris approaches the scleral spur, it drops more posteriorly, creating the iris plateau configuration. Indentation gonioscopy will push the mid peripheral iris more posteriorly; however the ciliary body in these eyes is more anteriorly placed and resists posterior movement of the peripheral iris during indentation gonioscopy. In some cases, pharmacologic dilation of eyes with plateau iris may precipitate angle closure despite the presence of a patent laser PI. An additional laser procedure, a laser peripheral iridoplasty, may be corrective. UBM confirms the relatively flat iris approach toward the angle with a steeper peripheral descent of the iris toward the scleral spur (Figure 9.5).9 Iridociliary body cysts may cause a plateau iris-like configuration (Figure 9.6).10
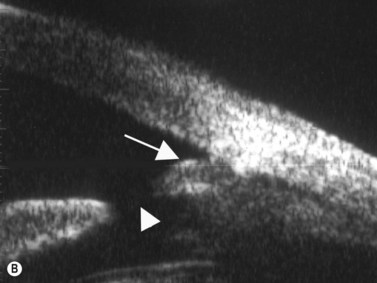
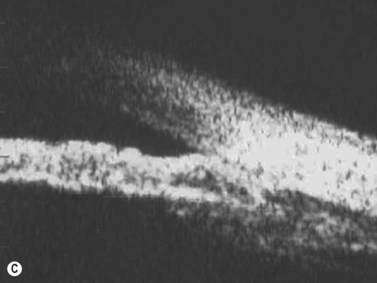

Reproduced with permission from: Rockwood EJ, Sharma S, Hayden BC, Singh AD. Glaucoma. Ultrasound Clin 2008; 3(2):207–215.4 Angle appearance before (C) and after (D) laser iridoplasty. Note separation of peripheral iris from the trabecular meshwork (D, arrow). C and D courtesy of M. Willet, MD and J Eisengart, MD, Cleveland, Ohio.