anatomy and provide a basis for the evaluation of congenital vascular abnormalities (Table 10.1).
TABLE 10.1 Abnormal Course of Support Devices Suggesting Vascular Anomalies or Congenital Heart Disease | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
and IV access. For example, the injection rate of ˜1.0 mL/s can be used in infants. For adult-sized older children, the contrast can be injected at 3 to 5 mL/s. The antecubital location is the preferred access site for the larger vein size needed to accommodate high flow rates of IV contrast administration for CTA. In neonates and young infants, a forearm, hand, or foot vein may also be considered. In such cases, the use of a power injectable, peripherally inserted central catheter is a more desirable and safer option.4 On the basis of hemodynamic and anatomic data, the injection of IV contrast medium should be performed into the right upper extremity vein in order to limit streak artifacts from the dense contrast across the aortic arch, which can occur when the left upper extremity vein is used9 (Table 10.2). Initially, the test injection should be performed using peripheral IV access with saline with a flow rate similar to that planned for the contrast medium for CTA. If the test injection is uneventful, the contrast injection, followed by a saline chase to clear the venous inflow and optimize the volume of contrast medium that reaches the target region, can be subsequently obtained.
TABLE 10.2 Recommended Intravenous Catheter Sites in Relation to Anatomy | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
with the nulling of flowing blood and may appear bright on the sequence, potentially resulting in artifacts that may lead to misinterpretation. For this reason, gadolinium should be administered only after black-blood imaging has been performed.14 T1-weighted gradient echo sequences performed before and after contrast administration are usually used instead of black-blood MR images for the assessment of vessel wall thickening in cases of vasculitis.15
TABLE 10.3 Cardiovascular Advanced Visualization Techniques | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
ascending aorta before giving origin to the right and left pulmonary arteries, which are derived from the sixth pharyngeal arch. The left pulmonary artery (LPA) is shorter and slightly smaller than the right pulmonary artery (RPA). The ductus or its remnant, the ligamentum arteriosum, courses posteriorly and superiorly to the undersurface of the aortic arch just distal to the origin of the left subclavian artery. The RPA and LPA travel along the bronchi down to the subsegmental level matching the adjacent bronchi in course and caliber.22,29,30,31
 FIGURE 10.1 Normal aortic segments with standard landmarks for reporting aortic diameter. Locations: (1) sinuses of Valsalva; (2) sinotubular junction; (3) midascending aorta; (4) proximal aortic arch; (5) midaortic arch; (6) proximal descending thoracic aorta (begins at the isthmus); (7) middescending aorta; (8) aorta at diaphragmatic hiatus; (9) abdominal aorta at the celiac axis origin. (Based on Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Catheter Cardiovasc Interv. 2010;76[2]:E43-E86. Ref. 15.) |
right common carotid artery, the left common carotid artery, the left subclavian artery, and the aberrant right subclavian artery, which takes a retroesophageal course. This vascular anomaly does not form a vascular ring because the trachea and esophagus are not entirely surrounded by vessels and/or ligaments. In the older literature, the presence of this variant was reported to result in so-called dysphagia lusoria in elderly patients. In these cases, the aberrant right subclavian artery is smooth in its contours, nearly equal in caliber throughout its intrathoracic course and tapers gradually37,38,39 (Fig. 10.3).
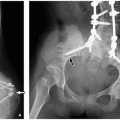
 FIGURE 10.2 Cervical aortic arch in a 3-year-old girl who presented with a pulsatile left upper chest mass. A: Frontal chest radiograph shows a superior mediastinal lesion (arrows). B: Axial enhanced CT image demonstrates a left aortic arch (arrow) which is located in a supraclavicular region. |
 FIGURE 10.3 Left aortic arch with an aberrant right subclavian artery in a 2-month-old boy who presented with intermittent stridor. A: Lateral view of esophagogram shows mass effect (arrow) upon the posterior aspect of the barium containing esophagus. B: 3D volume-rendered CT image demonstrates an aberrant right subclavian artery (arrow), which is smooth in caliber and without evidence of a Kommerell diverticulum or airway compression. However, the compression on the esophagus (E) is again seen. |
TABLE 10.4 Surgical Management of Symptomatic Vascular Rings | ||||||
|---|---|---|---|---|---|---|
|
 FIGURE 10.4 Double aortic arch. Ao, ascending aorta; LCCA, left common carotid artery; LSA, left subclavian artery; PA, pulmonary artery; RCCA, right common carotid artery; RSA, right subclavian artery. |
Right aortic arch with an aberrant left subclavian artery off a Kommerell diverticulum
Right aortic arch with left descending aorta (right circumflex aortic arch) (Fig. 10.7)

FIGURE 10.5 Double aortic arch with a dominant right arch and a smaller left arch with an atretic segment in a 2-year-old girl who presented with a history of recurrent pulmonary infections and an abnormality on chest radiograph. A: Frontal chest radiograph shows mild deviation of the trachea (asterisk) to the left with an indentation (arrow) on the right lateral wall of the trachea suggesting a right sided aortic arch. B: Lateral esophagogram image demonstrates a posterior indentation (arrow) with narrowing of the esophagus. C: Posterior view of 3D volume-rendered CT image shows a double aortic arch with a dominant right arch (RA) and a smaller left arch with an atretic segment (arrow). (DA, descending aorta.) 3D volume-rendered CT images facilitate evaluation of arch dominance and location.

FIGURE 10.6 Double aortic arch in an 18-month-old boy who presented with progressively worsening stridor. A: Axial enhanced CT image shows symmetric origins of the four arch vessels (white arrows), also known as “four-vessel” sign, arising separately from the two aortic arches. (RCCA, right common carotid artery; RSCA, right subclavian artery; LCCA, left common carotid artery; LSCA, left subclavian artery). Both aortic arches are nearly equal in size and encircle the narrowed trachea ( yellow arrow). B: Superior view of 3D volume-rendered CT image demonstrates the characteristic vascular anatomy of a double aortic arch to better advantage. In this instance, the right (R) and left (L) aortic arches have relative codominance, forming a complete vascular ring. C: 3D volume-rendered CT image shows the marked tracheal compression (arrows) at the level of the double aortic arch.

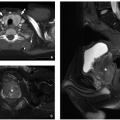
FIGURE 10.7 A circumflex aortic arch in a 5-year-old boy who presented with dysphagia and an abnormal esophageal impression on barium swallow study. Axial double inversion recovery MR images at the level of the right-sided aortic arch (A) and more inferiorly (B) show a right aortic arch (RA) and the descending portion (DA) of the circumflex aorta located to the left of the spine, indicating that there is a vascular ring. T, trachea. C: 3D volume-rendered CT image shows the circumflex aorta (arrow) coursing from right to left.

FIGURE 10.8 Right aortic arch with an aberrant left subclavian artery. Asc AO, ascending aorta; LCA, left common carotid artery; LPA, left pulmonary artery; LSCA, left subclavian artery; MPA, main pulmonary artery; RCA, right common carotid artery; RSCA, right subclavian artery.
Right aortic arch with mirror-image branching and a left retroesophageal ductus arteriosus or ligamentum arteriosum (Fig. 10.8)
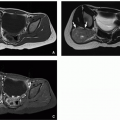
 FIGURE 10.9 Right aortic arch with an aberrant left subclavian artery off a Kommerell diverticulum in a 5-month-old girl who presented with worsening stridor. A: Axial enhanced CT image shows a right aortic arch (RA) with a Kommerell diverticulum (arrow). Trachea (T) compression is also seen. B: 3D volume-rendered CT image demonstrates an aberrant origin of the left subclavian artery (arrow) off a Kommerell diverticulum (asterisk). The Kommerell diverticulum (asterisk) is larger in caliber than the subclavian artery (arrow) because it represents a remnant of the ductus arteriosus that once carried much of the systemic blood flow during fetal life. The atretic portion of the ligamentum arteriosum completes the ring, but is not visible with current CT techniques. RA, right aortic arch. C: Coronal external volume-rendered CT image of the airways and lungs shows the narrowing (arrow) of the trachea because of underlying vascular ring. |
progressively courses into the left before reaching the aortic hiatus.
 FIGURE 10.10 Right aortic arch with left descending aorta (right circumflex aortic arch) in a 3-month-old boy who presented with increasing respiratory distress. Posterior view (A) and cranial view (B) of 3D volume-rendered CT images show a right-sided aortic arch (RA). There is also a prominent, patent ductus arteriosus (PDA) completing the vascular ring. Note that the aberrant left subclavian artery (LSCA) originates from the PDA. (RSCA, right subclavian artery.) |
abnormal vasculature and adjacent airway. Furthermore, the multiplanar and 3D reformatted CT images may aid in differentiation between pulmonary agenesis, pulmonary aplasia, and severe pulmonary hypoplasia by better depicting the bronchial stump and/or rudimentary bronchial tree47,50,53 (Fig. 10.12).
 FIGURE 10.11 Right aortic arch with mirror image branching in a 5-year-old boy who presented with abnormal chest radiograph obtained for evaluation of pneumonia. Axial white-blood (A) and coronal 3D volume-rendered (B) MR images show a right aortic arch (RA) with mirror image branching. First branch, innominate equivalent with a common trunk (straight arrow) for the left common carotid and left subclavian artery, followed by the right common carotid artery (curved arrow) and right subclavian artery (arrowhead) are seen. |
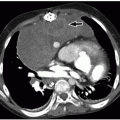
 FIGURE 10.12 Pulmonary agenesis in a 15-year-old girl who presented with worsening asthma. A: Frontal scout CT image shows marked hyperinflation of the left lung that extends across the midline anteriorly and herniates toward the right. There is dextroposition of the heart into the right hemithorax. B: Coronal posterior view 3D volume-rendered CT image of the central airways and lungs demonstrates complete agenesis of the right bronchus and lung. A normal left mainstem bronchus (arrow) is seen. C: Axial 3D volume-rendered CT image also shows dextroposition of the heart and compensatory hyperexpansion of the left lung, particularly of the left upper lobe (asterisks), which herniates into the right hemithorax. |
and flu vaccinations during the winter months should be given to affected children with substantial underlying lung deficiency. In infants under the age of 2, some authors advocate preventive care with palivizumab during the respiratory syncytial virus season.49 In rare instances, when the associated cardiovascular anomalies result in substantial airway compromise, surgery may be required.49,50
II PAS is characterized by a more inferiorly positioned carina at the level of T6. Type II PAS is usually associated with long-segment tracheal stenosis with complete cartilaginous rings and abnormal bronchial branching, including an inverted T-shaped carina and a right-bridging bronchus.50,56,58
 FIGURE 10.13 Pulmonary artery sling. The left pulmonary artery (LPA) arises from the right pulmonary artery (RPA) and courses between the trachea and the esophagus while entering the left hilum. MPA, main pulmonary artery. |
 FIGURE 10.14 Pulmonary artery sling in a 2-day-old boy who presented with severe respiratory distress. A: Axial enhanced CT image shows that the left pulmonary artery (asterisk) originates from the proximal right pulmonary artery (RP) before crossing behind the rounded trachea (arrow) to feed the left lung. B: Coronal 3D volume-rendered CT image shows severe distal tracheal narrowing (arrow) at the level of the aberrant course of the left pulmonary artery (LPA). The distal trachea (asterisks) shows long segment stenosis from complete tracheal rings. Also present is a T-shaped carina. |
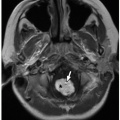
 FIGURE 10.15 Pulmonary artery sling in a 3-day-old girl who died of complications of tracheal atresia (with complete distal rings) and pulmonary hypoplasia. The left pulmonary artery (arrow) branches off a dilated pulmonary trunk and courses posterior to the narrowed trachea (T). In this example, the right lung is attached to the left lower lobe (“horseshoe lung”) (asterisk). |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


