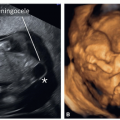
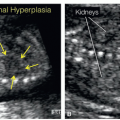
techniques, is essential to ensure uniformity of NT measurements among various operators.13 NT image criteria have been developed for adequate measurements (Fig. 1.1).14,18 Semi-automated methods of measuring NT thickness have also been developed by several ultrasound manufacturers in order to reduce operator-dependent bias in NT measurements (Fig. 1.2).19 Table 1.1 summarizes the essential criteria for an adequate NT measurement. The role of NT in detecting fetal aneuploidies is discussed in Chapter 6.
 Figure 1.1: Midsagittal view of a fetus at 13 weeks of gestation showing the nuchal translucency (NT) thickness measurement according to the recommended standards as listed in Tables 1.1 and 1.7. The schematic diagram in the figure shows the correct (C) and incorrect (A, B, D) placement of the calipers for NT measurements. In this example the NT measurement is 2.2 mm. |
Table 1.3 summarizes essential criteria for the adequate assessment of ductus venosus Doppler waveforms.
 Figure 1.2: Midsagittal view of a fetus at 12 weeks of gestation showing the semiautomatic measurement of the nuchal translucency (NT) thickness. In the semiautomatic approach, the examiner places a box around the region of interest (dash box) and the software recognizes the largest NT size and places the calipers accordingly. This approach decreases the subjectivity of the measurement and increases its accuracy. In this example the NT measurement is 2.1 mm. |
Table 1.1 • Criteria for the Standardized Measurement of Nuchal Translucency (NT) According to the Fetal Medicine Foundation-United Kingdom14 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


