he Pediatric Vertebral Column: Alterations in Bone Structure
10.1055/b-0034-87916
The Pediatric Vertebral Column: Alterations in Bone Structure
Increased Density
Generalized Increased Density
Please note that humans are not densitometers; we are only recognizers of interfaces. Plain image recognition of increased or decreased density is only possible in relation to adjacent objects.
Sclerosis of the vertebrae can occur in all diseases in which generalized sclerosis of all bones occurs.
Table 4.102 Generalized increased density
Diagnosis
Findings
Comments
Physiologic “bony sclerosis of the neonate”
Apparent increased density of multiple bones, decreasing in the first weeks of life. One explanation is the difference from prenatal bone and the metaphyseal less dense bone created in the first weeks of life. See below for bone-in-bone appearance.
Can closely mimic osteopetrosis. True increased density is in relation to neighboring structures, such as zones of provisional calcification or tooth buds. Bones can be made more or less dense on picture archiving and communication system (PACS) with maneuvering.
Diffuse sclerosis systematically of all or part of the vertebral bodies and entire skeleton. “Rugger jersey” spine in some older children.
Anemia occurs when too much bone is involved. Increase bone fragility, even in vertebrae. Occasionally has multiple wormian bones. May have jaw osteomyelitis. Osteocytic osteolysis impairment may be a cause.
Bone marrow hyperplasia
Dense trabeculation. If severe, could show extramedullary hematopoiesis.
Chronic iron deficiency and hemolytic anemias, and particularly thalassemia major. MRI shows well the abnormal pattern vs. expected fat in marrow.
Pyknodysostosis
Generalized sclerosis.
Bone fragility. Multiple wormian bones. Short stature. Toulouse-Lautrec’s syndrome is a possible example.
Fluorosis
Generalized sclerosis is systematically laid down in bone during exposure.
Osteoporosis can also occur in chronic fluoride intoxication.
Diaphyseal vigorous periosteal reaction leads to sclerotic appearance. In vertebrae, mainly seen in the neural arch.
Also know as Camurati-Engelmann disease. Increased uptake in bone scintigraphy in a ctive stage. Similar pattern in mother-of-pearl industrial exposure.
Osteomesopyknosis
Density similar to osteopetrosis, but limited to trunk and the most proximal limbs.
May have back pain.
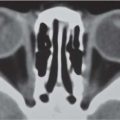
Fig. 4.268 Osteopetrosis in a neonate (compare to Fig. 4.192). Denser than normal bones and prominent vascular clefts are noted.Fig. 4.269 Camurati-Engelmann disease. The neural arches are dense compared to the bodies, as are regions in the ilium. These are analogous to the periosteal reaction of the dense femoral shafts (arrow). The density remains normal in femoral epiphysis (E) and metaphysis, as well as the vertebral bodies. All but the most posterior parts of the posterior ribs also dense.
Table 4.103 Bandlike sclerosis
Diagnosis
Findings
Comments
Bone-in-bone appearance
Normal growth pattern in the very young.
Normal in neonates and prematures in the first 2–8 wk. Evolves to normal spontaneously.
Healing osteoporosis
Newest normal density bone interfaces with osteoporotic bone.
A characteristic of osteopetrosis and osteomesopyknosis.
Healing renal osteodystrophy
Band of normal bone looks denser than earlier demineralized bone.
Chronic lead poisoning
Dense bands less conspicuous than those of long bones.
Also in bismuth poisoning.
Idiopathic hypercalcemia and hypervitaminosis D
Bands of increased density during the metabolically active period of the conditions.
Occasionally, hypervitaminosis D leads to less than normal density instead.
Fig. 4.270 Harris lines. Osteoporotic vertebral bodies show dense thin lines (growth arrest/recovery lines of Harris or Park) paralleling the end plates. This teenager with Duchenne muscular dystrophy has had a heart transplant and thus receives periodic metabolic jolts from immune therapy, resulting in the lines.Fig. 4.271 “Rugger jersey” in osteopetrosis in a 1-year-old girl. The metaphyseal equivalents adjacent to the end plates are denser than the central (older) portions of the vertebral bodies. A dense 12th rib is noted (arrow).
Table 4.104 Localized sclerosis
Diagnosis
Findings
Comments
Bone island (s)
Homogeneous, often round, sclerotic, with hazy borders.
Also called osteomas. Of no clinical significance, except diagnostically if part of Gardner syndrome.
Sclerotic pedicle
Contralateral to spondylolysis. Possibly metastasis.
Predominantly increased density of the affected vertebral bodies.
Marrow replacement on MRI.
Ewing sarcoma
Mostly sclerotic, arch or body.
Hemangioma
Dense and coarse trabeculae.
Often asymptomatic. Nicely shown on thin-section CT.
Metastases from medulloblastoma
Or retinoblastoma.
Osteogenic sarcoma
Unusual in vertebral location.
Chordoma
Mainly in clivus or sacrum.
Endosteal hyperostosis
Cortex of pedicles and other arch elements is thick at expense of medullary cavity; sclerotic calvarium and jaw.
Worth type is AD; van Buchem type is autosomal recessive.
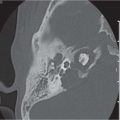
Fig. 4.272 Osteoid osteoma in the pars articularis of L4. A 14-year-old girl with back pain and scoliosis (note tilt of L3).Fig. 4.273 Osteoid osteoma seen on axial CT at the medial right pedicle (on bone scan the lesion was hot). Moderately severe associated scoliosis is reflected by the rotation of the vertebra in the axial plane.Fig. 4.274a–d Non-Hodgkin lymphoma. (a) Radiograph with increased density of S2 on the right. (b) Classic bone scintigram with increased uptake in the right sacrum, view as from behind. (c, d) CT of the sacrum with sclerosis on the right.
Only gold members can continue reading. Log In or Register to continue