Sinusitis—acute and chronic |
Radiograph/CT/MRI: homogeneous opacification, mucosal swelling or air-fluid levels.
May see bony sclerosis or destruction if chronic. |
CT important to assess for anatomic variations prior to functional endoscopic sinus surgery. Use low-dose coronal scans. Also useful to look for complications. |
Trauma
Fig. 4.140 |
Radiograph: soft-tissue swelling, maxillary sinus opacification, ± air-fluid level.
CT: axial and coronal planes to visualize fracture. |
|
Polyp/retention cyst |
Radiograph: Opacification of single maxillary antrum. Soft-tissue mass in anterior nasopharyx on lateral view.
CT: homogeneous soft-tissue masses with smooth margins, outlined by air (e.g., mucocoele). |
Sequelae of sinonasal inflammation. |
Tooth bud |
Radiograph: usually caused by projection and overlap.
CT: shows true ectopic tooth bud within maxillary sinus. |
|
Osteoma |
Radiograph/CT: well-defined bony density. Mainly in frontal sinuses; rarely ethmoid and maxillary. |
Assess for Gardner syndrome. |
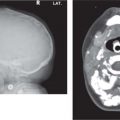
Mucocoele
Fig. 4.141 |
CT/MRI: appearance varies with water and mucoid content. Shows peripheral enhancement, distinguishing it from neoplasm. Exhibits mass effect on adjacent structures and often expands into orbit. |
Due to obstruction of sinus ostium. Most commonly frontal and ethmoid sinuses. |
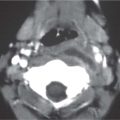
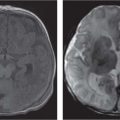
Primary malignancy
Fig. 4.142a, b |
CT/MRI: MRI preferred due to superior soft-tissue contrast and to show intracranial extension. Need pre- and postcontrast studies. |
Lymphoma, rhabdomyosarcoma, nasopharyngeal carcinoma, malignant histiocytoma. |
Metastases |
CT: usually neuroblastoma and is associated with soft-tissue mass. |
|
Juvenile angiofibroma |
CT: isointense or low-density mass with widening of pterygopalatine fossa and bowing of posterolateral maxillary sinus. Marked CE.
MRI: T1 hypointense, T2 hyperintense with flow voids and avid enhancement. Can show cysts, cavitation, and hemorrhage. |
Benign, most common in adolescent boys. |
Osteomyelitis |
Radiograph/CT: sclerosis and destruction of sinus wall in setting of infection. |
Usually frontal sinus. |
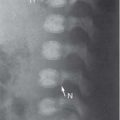
Fibrous dysplasia
Fig. 4.143 |
CT: depends on fibrous vs. osseous component. Varies from radiolucent to ground-glass.
Unilocular/multilocular lesion, well-defined margin.
MRI: sharply demarcated mass, variable signal intensity, diffuse CE. |
|
Ossifying fibroma
Fig. 4.114, p. 369
Fig. 4.138, p. 381 |
CT/MRI: expansile lesion with prominent areas of nonossified fibrous tissue.
Can be lytic, expansile containing calcification, and show cortical erosion. |
|