Normal: anterior buckling (expiration±flexion) in the ear lobe |
Lateral radiograph: “pseudothickening”—if neck not adequately extended or flexed may get artificially thickened soft tissue in younger children. |
|
Adenoid tonsil
Fig. 4.144 |
Lateral radiograph: soft-tissue pad in posterior nasopharynx causing narrowing of airway. Sagittal MRI: Soft-tissue mass in nasopharynx. High signal on T2. |
If enlarged, causes obstructive sleep apnea.
If > 12 mm, it is abnormal. |
Palatine tonsil
Fig. 4.145 |
Lateral radiograph: prominent soft-tissue mass overlying posterior inferior aspect of soft palate.
MRI: bilateral enlarged high signal masses on T2. |
If enlarged, causes obstructive sleep apnea. |
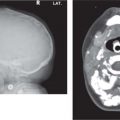
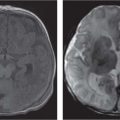
Trauma/hematoma ± fracture
Fig. 4.146 |
Lateral radiograph: prevertebral soft-tissue swelling is greater than the width of vertebral body ± fracture, ± spondylothesis. Atlas dens interval (ADI) may be > 5 mm. Basion-dens interval may be > 12 mm. Power ratio > 1 in atlantoccipital dissociation. Sagittal MRI: prevertebral soft-tissue swelling/hematoma. Retroclival hematoma and blood between basion and dens implies apical/alar ligament disruption. Check tectorial ligament and posterior ligaments. May have associated cord edema. |
Prepontine blood seen on NECT should alert to possible cervical spine injury with retroclival hematoma; urgent MRI is indicated even in face of normal lateral cervical spine radiograph. |
Epiglottitis |
Lateral radiograph: (patient upright) enlargement of epiglottis and thickening of aryepiglottic folds.
CT (rarely indicated): enlarged, edematous epiglottis and aryepiglottic folds. |
Medical emergency—complete airway obstruction may occur at any time. “Thumb” sign. |
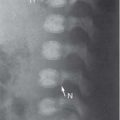
Retropharyngeal abscess
Fig. 4.147
Fig. 4.148 |
Lateral radiograph: widening of retropharyngeal soft tissue, ± gas, or air-fluid level. Loss of normal cervical lordosis.
CECT: identifies extent of disease and drainable collections, which are hypodense with rim enhancement. |
Cellulitis more common than abscess.
Mass effect on the airways may cause respiratory compromise. |
Foreign body |
Lateral radiograph: only if radiopaque. |
May require contrast swallow postremoval to check for leak. |
Lingual thyroid |
CT: hyperdense, well-circumscribed mass at base of tongue that enhances strongly with contrast.
MRI: T1—increased signal compared to tongue.
T2—increased signal.
Enhances with contrast.
Nuclear medicine (NM): positive technetium-99m pertechnetate uptake confirms ectopic thyroid. |
A 1–3 cm well-circumscribed, round/ovoid, midline/paramedian tongue base mass.
Important to look for normal cervical thyroid tissue, which may be absent. |
Lymphadenopathy |
US: oval homogenous nodes of varying sizes, ± central hypoechogenicity if forming abscess
CECT: well-defined homogenous masses with variable enhancement; ± linear enhancement of hilum of node; ± ring enhancement with hypodense center representing phlegmon or early abscess; ± perinodal fat stranding.
MRI: homogenous signal intensity unless suppurative. |
Nonneoplastic enlargement of nodes may be reactive or associated with infection.
Waldeyer ring may be enlarged.
Important to assess adjacent jugular vein for thrombosis. |