Radiotherapy (RT) plays a fundamental role in the treatment of tumors of the paranasal sinus and nasal cavity, in combination with surgery or as primary treatment, and can be combined with chemotherapy for inoperable cases. The great interest in proton and heavier charged particle therapy for paranasal sinus and nasal cavity tumors is related to the following:
▪ The irregular configuration of these tumors and their invasion into adjacent facial structures
▪ Their proximity to dose-limiting, critical normal tissues tissues including the ocular globes, optic nerves and chiasm, and brain, resulting in a high risk of associated late RT injury
▪ The relative radioresistance of some of these tumors, requiring high physical and biologically effective doses to achieve local control
▪ The high risk of local recurrence
▪ Data suggesting improved survival with aggressive local therapy
OVERVIEW
Epidemiology
Malignant tumors of the paranasal sinuses and nasal cavity are relatively rare, accounting for approximately 1% of all malignancies and 2% to 3% of all head and neck cancers with a yearly incidence of approximately one new case for every 100,000 people in the Western world. They are more common in men than in women with a ratio of 2:1 and appear more often after the age of 40, with the exception of esthesioneuroblastoma and lymphoma, which may occur before the age of 20.1 The most common site of origin is the maxillary sinus. Tumors arising in the sphenoid and frontal sinuses are very rare.
Pathology
A number of different tumor histologies can arise from the mucosa, soft tissue, and bony structures of the paranasal sinuses and nasal cavity.2 The most common histology in the maxillary sinus is squamous cell followed by adenocarcinoma (ACA), adenoid cystic carcinoma (ACC), and mucoepidermoid carcinoma. ACA, squamous cell carcinoma (SCC) and olfactory neuroblastoma are the most common histologies in the ethmoid sinus. Other tumor types originating from paranasal sinuses and nasal cavities are sarcomas and melanoma. According to the pathologic type, location, and stage, these tumors can have a different natural history with respect to nodal involvement and distant metastases, requiring specific treatment approaches.
Natural History
Carcinomas arising in the ethmoid sinus and upper nasal cavity can invade the lamina papyracea, extend into the orbit, or invade the cribriform plate to extend into the anterior cranial fossa. Tumors arising in the lower aspect of the nasal fossae may invade the hard palate and the maxillary sinus. Carcinomas of the maxillary antrum arising in the suprastructure have a less favorable prognosis than those involving the infrastructure and may invade the orbit, pterygopalatine and infratemporal fossae, base of skull, ethmoid, and nasal cavity. Tumors arising in the infrastructure may extend to the hard palate, alveolar bone, subcutaneous soft tissue, and pterygopalatine fossa.
Diagnosis and Staging
Most tumors present in an advanced stage because of the often silent or nonspecific and mild symptoms of early disease, which mimic those of chronic sinusitis. The early symptoms, that is, headaches, facial pain, intermittent epistaxis, and nasal stuffiness, often result in diagnostic delays. Symptoms associated with advanced stage disease include upper gingival pain, trismus, nasal discharge, anosmia, diplopia, facial asymmetry with subcutaneous swelling, and multiple cranial nerve deficits. For tumor staging, the International Union Against Cancer/Americal Joint Committee on Cancer (UICC/AJCC) system is most commonly used.3 A specific staging system has also been proposed for esthesioneuroblastoma (the Kadish et al.,4 and the University of California at Los Angeles [UCLA] Dulguerov and Calcaterra5 classifications) and melanoma.6
The diagnostic evaluation to assess the extent of locoregional disease should include flexible fiberoptic endoscopy and imaging studies. Computed tomography (CT) and magnetic resonance imaging (MRI) are the most used diagnostic modalities to detect bone involvement and invasion of surrounding structures. The discrimination of tumor from adjacent tissues and retained secretions can be assessed with MRI, obtaining T2-weighted and T1-weighted (with and without gadolinium enhancement) sequences. Fat-saturated T1-weighted sequences after contrast administration and three-dimensional (3-D) volumetric interpolated breath-hold examination (VIBE) sequences have also been recommended to assess perineural spread as well as subperiosteal bone and fat invasion.7 Positron emission tomography-computed tomography (PET-CT) is under investigation for these as well as for other head and neck tumors.8 Metastatic workup has traditionally included chest CT (including liver) and bone scan, although the bone scan has been supplanted at some institutions by the PET scan and more recently by PET-CT.
General Management
Surgical resection, as complete as possible, has been associated with a higher tumor control probability9,10 in most histologic types and should be performed whenever possible. Owing to the usual extent of these tumors and the difficulties in achieving an R0 (margin-negative) resection, surgery is usually combined with RT, especially for locally advanced lesions. The development of more conformal RT techniques has led to a more conservative surgical approach for patients with orbit involvement. Chemotherapy can also be used in conjunction with RT and surgery for management of selected, locally advanced histologic types.
ADVANTAGES OF CHARGED PARTICLE THERAPY
Tumors of the paranasal sinuses and nasal cavity are well suited for proton or heavier charged particle therapy. The physical properties of charged particles allow the optimal conformation of dose to these irregularly shaped tumors adjacent to so many critical, radiation-sensitive normal tissues. The relative radioresistance of some of these tumors requires high physical dose to achieve local control. For unresectable tumors or patients with gross residual disease after resection, there may be an additional benefit for higher biologically effective doses (i.e., carbon ion therapy).
Comparative Treatment Planning Studies
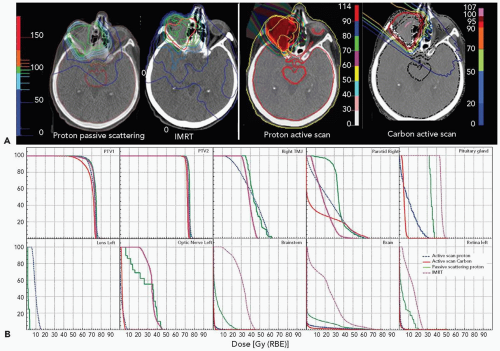
The theoretical advantage of protons and ions over photons for increasing the tumor control probability and decreasing the risk of normal tissue complications has been demonstrated in multiple treatment planning comparisons (see Table 16A.1). In all of these studies, proton or carbon ion therapy alone or in conjunction with conformal photons, applied with 3-D or intensity-modulated techniques, proved to be superior in limiting the dose to critical structures for similar target volume coverage compared to photons with or without intensity modulation.11, 12, 13, 14 Intensity-modulated proton beams provide an even better physical dose distribution than passively scattered proton beams for tumors involving the skull base.14,15
Moreover, protons and ions are able to reduce the dose to critical structures with similar or superior coverage of the target volume using fewer fields than photon treatment (see Fig. 16A.1). In this way, protons can reduce the integral dose, that is, the volume receiving a low but non-negligible dose, with the potential for reduction in both early and late side effects, including the risk of a secondary neoplasm. Because of these favorable dosimetric characteristics, a higher radiation dose (RT) can also be delivered to the target volume, leading to better local tumor control for any given normal tissue complication probability.
CLINICAL RESULTS
Proton Therapy
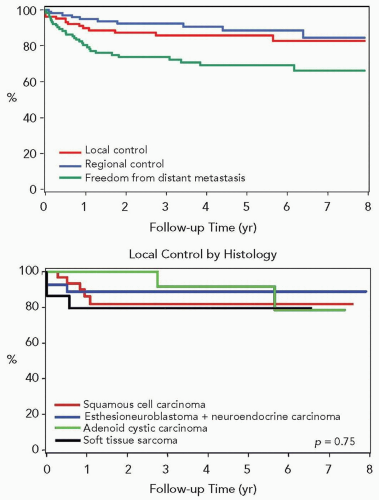
Significant experience with proton therapy for paranasal sinus tumors has been reported from the Massachusetts General Hospital (MGH), Boston, MA.16 Between 1991 and 2002, a total of 102 patients with advanced sinonasal lesions received proton beam radiotherapy at the Harvard Cyclotron Laboratory (HCL). There were 33 squamous cell carcinomas, 30 esthesioneuroblastomas and carcinomas with neuroendocrine differentiation, 20 ACCs, 13 soft tissue sarcomas, and 6 adenocarcinomas. Thirty-three percent of patients received chemotherapy, which consisted mainly of induction chemotherapy. With a median follow-up of 44 months, 12 and 26 patients developed local recurrence and distant metastasis, respectively, as their first sites of failure (see Fig. 16A.2A). Distant metastasis was the predominant pattern of relapse for squamous cell carcinoma, carcinoma with neuroendocrine differentiation, and ACC. At 5 years, overall survival (OS) and disease-free survival rates were 59% and 54%, respectively. The overall freedom from distant metastasis rate at 5 years was 69% (Fig. 16A.2). The 5-year actuarial local control rate was 86% (Fig. 16A.2). The local control rate at 5 years was 82% for squamous cell carcinoma and 90% for carcinoma with neuroendocrine differentiation (Fig. 16A.2).
The Proton Radiation Oncology Group (PROG) protocol 92-15 was launched for locally advanced paranasal sinus tumors using an accelerated, hyperfractionated schedule. For 91 cases treated to a median total dose of 73.6 Gy (RBE) (range 59.4 to 77.8 Gy [RBE]), the 5-year local control, OS and disease-free survival rates were 82%, 58%, and 52%, respectively, with differing outcomes according to the pathology.17 The proton therapy center in Kashiwa, Japan also recently reported preliminary data in 13 patients with esthesioneuroblastoma treated with protons alone or with surgery.18
Light Ion Therapy
The Lawrence Berkeley Laboratory was the pioneer for ion therapy (mostly with neon ions) in the treatment of paranasal sinus and nasal cavity carcinomas. Disease-specific survival and local control rates at 5 years were 69% in a group of 12 paranasal sinus cancer patients.19,20
Carbon Ion Therapy
National Institute of Radiological Sciences
The clinical experience with carbon ion therapy started in Chiba, Japan in 1994 at the National Institute of Radiological Sciences (NIRS). Following the outcome of a phase I Dose Escalation Study,21 a phase II Clinical Trial of Heavy Particle Radiotherapy was initiated in April 1997. A total of 227 patients corresponding to 230 lesions were registered from April 1997 to August 2005, including 60 patients with paranasal sinus and 53 with nasal cavity lesions of various histologies including malignant melanoma, ACC, ACA, and SCC. Five-year local control by histologic type was 77.0% for malignant melanoma, 73.9% for ACC, 70.2% ACA, 91% for ACA, and 66.3% for the 11 patients with SCC. The 5-year survival rate was 68.8% for ACC and 62.4% for ACA. The acute toxicity was very low (grade 3 skin and mucosa toxicity in 6.8% and 10.6% of patients, respectively and none worse than grade 3), and to date no late toxicities > grade 2 were reported. Subsequent trials are ongoing, including a phase I Dose Escalation Study for Bone and Soft Tissue Tumors of the Head and Neck and a phase II Clinical Trial of Carbon Ion Radiotherapy Combined with Chemotherapy for Mucosal Malignant Melanoma of the Head and Neck.22
Gesellschaft Für Schwerionenforschung
Carbon ion RT has been available since December 1997 at the Gesellschaft für Schwerionenforschung (GSI), in Darmstadt, Germany. The dedicated medical fixed horizontal beam line for carbon ion therapy has been available for three treatment bocks annually, with each block consisting of 20 consecutive days. A series of 152 cases of head and neck tumors treated by carbon ions at GSI-Deutsches Krebsforschungszentrum (DKFZ) in Darmstadt-Heidelberg was reported by Schulz-Ertner et al.23 Twenty-one patients with ACCs in various primary locations including paranasal sinuses were treated with a combination of stereotactically guided photon RT and a carbon ion boost to a total dose of 72 Gy (RBE). The 4-year actuarial local control and OS rates were 77.5% and 75.8%, respectively.23
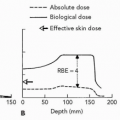
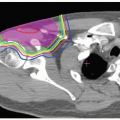
Figure 16A.1 Comparative dosimetric analysis evaluating intensity-modulated radiotherapy (IMRT), actively scanned protons, passively scattered protons, and scanned carbon ions. A: Figures show comparative dose distributions, comparing IMRT, passively scattered protons, scanned protons, and scanned carbon. B: The figures show comparative dose-volume histograms (in % volume versus dose) for respective organs. PTV, planning target volume; TMJ, temporomandibular joint. Reprinted with permission from Krengli M, Bourhaleb F, Cozz iL, et al. Treatment planning comparison of photon IMRT, active and passive proton therapy, and carbon ion therapy for treatment of head and neck tumors. Int J Radiat Oncol Biol Phys. 2006;66(3):S669.
TECHNICAL ASPECTS OF TREATMENT
Immobilization and Setup
Patients are treated in a position that maximizes the daily setup reproducibility. They are generally secured in a supine position with an immobilization mask, extended to the shoulders if neck RT is planned. A system using dental fixation with a bite block to protect the tongue and oral mucosa and a thermoplastic mask has been developed and tested by the MGH.24 The mask and bite block are pinned to the frame allowing a repositioning of the patient in three translational and three rotational degrees of freedom. The University of Heidelberg developed a rigid mask system consisting of a cast made of selfhardening bandages attached to a stereotactic frame.25 At the NIRS, patients are positioned in customized cradles and immobilized with thermoplastic masks. Day-to-day uncertainty for positioning and fixation in these devices, however, was reported to be 1.8 to 2.3 mm, making mandatory the use of systematic pretreatment verification radiographs when high accuracy is needed.
Patient Data Acquisition
Target volume definition is based on imaging studies including CT and MRI. The use of PET-CT images for target delineation is under investigation. CT and MRI images with contrast enhancement should be performed in the immobilized treatment position indexed every 3 mm extending from the vertex of the skull to the clavicular heads. Afterwards, CT and MRI images are sent to the 3-D treatment planning system and fused by dedicated image fusion software.
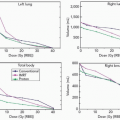
Figure 16A.2 The upper graph shows local control, regional control, and freedom from distant metastases in patients treated at Massachusetts General Hospital (MGH) with high-dose photon/proton RT for locally advanced paranasal sinus tumors. The lower graph shows local control in patients treated at MGH with high-dose photon proton RT according to histology. Reprinted with permission from Chan AW, Pommier P, Deschler DG, et al. Change in patterns of relapse after combined proton and photon irradiation for locally advanced paranasal sinus cancer [Abstract]. Int J Radiat Oncol Biol Phys. 2004;60(1):S320.
Target Delineation
The gross tumor volume (GTV) is identified as the macroscopic disease detected by CT and MRI, with additional data from endoscopic examination as well as operative and pathologic reports in patients undergoing resection. The clinical target volume (CTV) expansion can be different in various directions depending upon the bony or soft tissue structures around the GTV and upon the width of the surgical margins in cases of postoperative RT. Special attention should be paid to possible cavernous sinus involvement, better delineated on MRI than CT. For maxillary sinus tumors, the entire ipsilateral maxillary sinus should be included in the CTV. In some cases, the tumor histology can also prompt a larger CTV; for example for T3-T4 undifferentiated tumors, the CTV should include the regional lymph nodes, and for ACC, the CTV should be extended to track potential perineural spread along the cranial nerves towards the base of skull.
The planning target volume (PTV) depends on the specific characteristics of the immobilization device and the procedure to control the accuracy of the daily setup. PTV margin expansion should be kept as low as possible to reduce the irradiation of the surrounding healthy tissues. For patients treated at GSI, the PTV for the carbon ion boost included the GTV with a 1- to 2-mm safety margin. At the NIRS, a 3- to 5-mm margin is used, but that could be reduced according to the surrounding organs at risk (OARs), whereas 2- to 3-mm aperture edge was added to the GTV for the boost with protons at the MGH.
Setup Verification—Image Guidance
Daily orthogonal pretreatment radiographs are performed and compared with digitally reconstructed radiographs, using cranial anatomic landmarks and/or on fiducial markers (gold) implanted in the skull (used routinely at GSI).
The β+ radioactive fragments generated from nuclear interactions along the beam path of particle beams can be imaged with positron emission tomography (PET) for setup verification.26 This is of particular importance in the treatment of paranasal sinus tumors, where the radiographic densities of the target volumes and surrounding tissues are very heterogeneous because of bone, air, and soft tissue and their interfaces. Therefore, minor inaccuracies in patient positioning or anatomic changes leading to local density modification (i.e., sinusitis, mucus retention in the sinus, or tumor regression over the course of treatment) may lead to underdosage of the target volumes and/or injuries to radiosensitive surrounding normal tissues.27
Irradiation Techniques
Several techniques have been designed for proton and carbon ion therapy according to the equipment available (limited in most centers until recently to fixed horizontal beams), the use of particle beams as an exclusive RT technique or combined with photons, and the experience and the ongoing protocols of each center (with regard to dose and fractionation).
Proton Therapy
Most clinical data for protons are at present based on 3-D conformal proton techniques. At the MGH, the RT strategy for locally advanced paranasal sinuses combined optimized photons (formerly 3-D conformal and now intensity modulated) and high-precision proton RT. For 3-D conformal photon RT, a five-field technique was used to design the treatment plan, consisting of an anterior and two sets of right and left lateral beams targeting the CTV. Photon dose was generally <20 Gy. These fields were matched to a lower anteroposterior neck field if required. Photon RT was delivered mostly with either 4 or 6 MV beams at MGH. Since January 2001, a pencil beam algorithm (XiO Treatment Planning System, CMS Medical Systems, St. Louis, MO) has been used for the dose calculation and provides a more accurate display of the dose in these regions, notably the effect of bony inhomogeneities. Before this, a broad beam algorithm was used. More recently, the photon component has been delivered by IMRT, with the capability to plan both the IMRT and proton components on the same treatment planning platform.
Carbon Ion Therapy
At GSI, patients with paranasal sinus cancers are treated with a combination of stereotactic photon RT (fractionated stereotactic or intensity-modulated stereotactic RT) to the CTV and a carbon ion boost to the GTV. Treatment planning for carbon ion RT includes biologic plan optimization using the treatment planning for particles (TRiP) treatment planning software based on the Local Effect Model. Plans consist of two to three isocentric fields. An intensity-modulated beam delivery system based on the raster scanning technique developed at GSI enables precise delivery of the carbon beams to the target.
At NIRS, patients with head and neck cancer were irradiated exclusively with carbon ions. Ongoing protocols are assessing the role of concomitant chemotherapy in patients with mucosal melanoma. Patch field techniques were used in some patients to avoid an overdose to the surface of critical organs. A dosimetry system for heavy ion RT was established to deliver heavy ion doses safely to the patients according to the treatment plan.28
Dose, Fractionation, and Dose Constraints
The dose prescribed to the PTV or to the different PTVs can be established based on a few parameters—the presence of macroscopic disease, the margin status after surgery, and the histologic type. On the basis of data from photon RT and the accumulated proton experience, the following dose levels (at standard fractionation) have been proposed:
▪ Definitive RT or postoperative RT for macroscopic residual disease: 70 to 75 Gy (RBE)
With regard to fractionation, daily fractions of 1.8 to 2.0 Gy, 5 days per week can be used for most cases. Hyperfractionation with or without acceleration has been explored with a combination of protons and photons at the MGH. Carbon ion protocols are generally based on hypofractionated schedules due to their radiobiologic properties (Chapters 2 and 10).
Protons (Massachusetts General Hospital Experience)
From 1991 to 2001, >100 patients with locally advanced tumors of different histologies were included in b.i.d. accelerated photon/proton RT protocols. The first scheme was an entirely b.i.d. program using 1.6 Gy (RBE) fractions, with a 6-hour minimum interfraction interval, 5 days a week, without any planned treatment breaks. The second RT scheme included an initial, conventionally fractionated q.d. schedule for 15 to 20 Gy (RBE) at 1.8 Gy (RBE) per session, followed by a b.i.d. program delivering 1.8 Gy (RBE) in the morning and either 1.4 Gy (RBE) or 1.5 Gy (RBE) in the evening, again with a minimum 6-hour interfraction interval. The total prescribed doses were 67.6 Gy (RBE) to the CTV encompassing areas with microscopically positive margins and other high-risk tissues and 76 Gy (RBE) to the GTV, with the exception of neuroendocrine tumors where 54 and 67.6 Gy (RBE) respectively were delivered to the GTV and CTV.
The optic nerves and chiasm were limited to 55.8 Gy (RBE) and the medial and posterior retina to 50.0 Gy (RBE) at <2.0 Gy (RBE) per day, whereas the brainstem surface was held to 64.0 Gy (RBE) at <2.4 Gy (RBE) per day. The dose constraint to the ipsilateral optic nerve was relaxed if tumor coverage was severely compromised. Although, there were no formal constraints on dose to brain tissue, it was recommended to keep the dose as low as achievable without compromising the target coverage.
Carbon Ions
Owing to the restricted availability of the medical carbon ion beam line for clinical patient treatment at the GSI facility, the protocols there were based on a combination of photons and carbon ions. The CTV was treated with photons to 54 Gy (at 1.8 Gy daily delivered in most cases with 5 to 7 beam IMRT) followed by a carbon ion boost of 18 Gy (RBE) in six consecutive daily sessions of 3 Gy (RBE) to the GTV plus a 1 to 2 mm margin. In the phase I NIRS protocols, two principal schemes were explored, delivering maximum doses of 70.2 Gy (RBE) in 18 fractions over 6 weeks or 64 Gy (RBE) in 16 fractions over 4 weeks, resulting in limited acute grade 3 skin and grade 2 mucosal toxicity. In the phase II clinical trial started in April 1997, the dose scheme was 64.0 Gy (RBE)/16 fractions/4 weeks (or 57.6 Gy [RBE]/16 fractions/4 weeks when a large volume of skin was included in the target volume).29
Toxicity—Organs at Risk
Optic Pathways
The radiation tolerance of the optic pathways is one of the main dose-limiting factors for paranasal tumor RT because of their close proximity to the tumors and the risk of vision loss when one exceeds tolerance. Prognostic factors for optic neuropathy have been widely described with photons. In the series of Parsons et al., no optic neuropathy or retinopathy was observed when the doses to these structures were respectively below 59 Gy and 45 Gy. The dose per fraction (>1.9 Gy) was also found as a prognostic factor for late toxicity above these doses.30,31 In a series from the MD Anderson Cancer Center, neuropathy was reported in only one case (at a dose of 56 Gy) when dose was limited to 60 Gy (median dose per fraction 2.2 Gy); they suggested that the maximum tolerated dose to the chiasm was 50 Gy (with median dose per fraction 2.0 Gy) and they estimated a 5% risk of chiasm injury for patients receiving 50 to 60 Gy. Corneal injury was significantly related to the total dose, dose per fraction, and the use of concomitant chemotherapy.32
Similar dose constraints have been adopted with conventionally fractionated protons, as described in the preceding text, for the dose fractionation employed in the MGH protocols. Weber et al. recently reported the visual outcome in patients with advanced sinonasal malignancies treated at MGH/HCL with photon/proton accelerated, fractionated RT.33 They analyzed 36 patients with full visual follow-up who were treated between 1991 and 2001 with a median dose to the GTV of 69.6 Gy (RBE) (range 60.8 to 77). The RT was usually given b.i.d. (interfraction interval of >6 hours) with a median photon fraction size of 1.8 Gy (range 1.6 to 2.0) and median proton fraction size of 1.6 Gy (RBE) (range 1.4 to 1.8). Thirteen patients developed late visual/ocular toxicity, including cataracts, grade 1 (two patients) and grade 3 (one patient), grade 1 vascular retinopathy (one patient), grade 1 optic neuropathy (one patient), nasolacrimal duct stenosis (grade 2 in two patients and grade 3 in one patient) and dry-eye syndrome (grade 1 in one patient and grade 2 in four patients). The 3- and 5-year probabilities of Late Effects of Normal Tissues/Common Toxicity Criteria (LENT/CTC) grade >2 visual toxicity were 15.8 ± 6.7% and 20.7 ± 7.8%.
Prognostic factors for optic injuries and correlative dose-volume histograms (DVHs) in patients treated exclusively with carbon ions have been detailed in 30 patients (54 optic nerves) by Hasegawa et al.34 No visual loss was observed when the maximal dose to the optic nerve was <57 Gy (RBE) compared to 58% when the maximal dose was higher. Interestingly, the dose received by 20% of the optic nerve was the only significant factor in a multivariate analysis.
Brain Toxicity
The risk of brain toxicity is also a major constraint for paranasal sinus RT especially for tumors originating or extending into the ethmoid sinus and/or into the base of the skull. In the MGH series of skull base chordomas and chondrosarcomas treated with high-dose photon/proton RT, only male gender was significantly associated with clinically symptomatic temporal lobe damage. Although radiation necrosis of the brain is usually not seen below 60 Gy with conventionally fractionated RT, the authors reported that necrosis could occur in patients in whom <10 mL of healthy brain parenchyma received higher than 50 Gy (RBE).35 Dose per fraction, overall treatment time, and altered fractionation have been reported as significant prognostic factors for temporal lobe necrosis in patients irradiated for carcinomas of the nasopharynx. The Biologically Equivalent Dose (BED) formula using an α/β ratio of 3 was described as an appropriate model for predicting late temporal effects.36,37
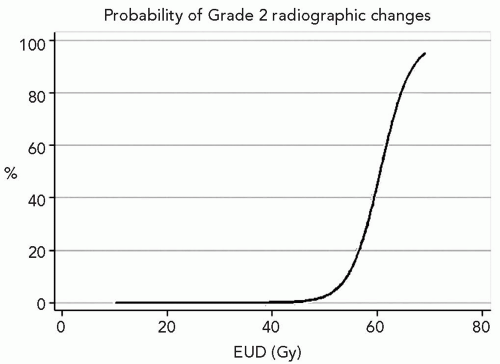
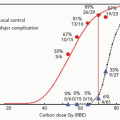
Figure 16A.3 Probability of > grade 2 brain necrosis according to the equivalent uniform dose EUD value in patients treated with high-dose combined photon and proton irradiation for paranasal sinus tumors. Reprinted with permission from Pommier P, Niemierko A, Adams J, et al. EUD predicts delayed hyperintensity on T1-weighted MRI after combined proton and photon irradiation in paranasal sinus cancer. Int J Radiat Oncol Biol Phys. 2004;60(1):S501-S502 and Niemierko A, Pommier P, Adams J, et al. Dose-volume characteristics of brain lobe late response following proton-photon radiotherapy of paranasal sinus cancer. Int J Radiat Oncol Biol Phys. 2005;63(1):S267.
The data from a systematic review of clinical and MRI outcomes in 53 patients treated with high- dose combined photon/proton RT for paranasal sinus tumors and followed for >18 months (median 5.4 years) have been analyzed for brain injury.38,39 The probability of brain necrosis was modeled using an equivalent uniform dose-based logistic method with a >90% predictive value for MRI outcomes (see Fig. 16A.3). Using this model, the estimated tolerance dose (D5%) for brain necrosis seen on MRI scans was approximately 60 Gy.
Several cases of brain injury were also reported in the experience of GSI with carbon ion therapy. In their chordoma/chondrosarcoma series, seven of 67 patients developed a contrast-enhancing lesion within the temporal lobes on MRI (with clinical symptoms in 3), related to the total target dose, noted in 5 of 10 receiving a target dose of 70 Gy (RBE) and 2 of 57 patients receiving between 57 and 65 Gy (RBE).23
MANAGEMENT OF SPECIFIC TUMOR HISTOLOGIES
Squamous Cell Carcinoma, Undifferentiated Carcinoma, and Adenocarcinoma
Squamous cell carcinoma is the most common histology seen in nasal cavity and paranasal sinus tumors, accounting for approximately 80% of cases; undifferentiated carcinoma (UC) and ACA are less common.
Typically, SCC and ACA are subclassified on the basis of the histologic grading from well to poorly differentiated, or even undifferentiated. The prognosis is worse for SCC and, in particular, for UC. In general, lymphatic spread to subdigastric, submandibular, and retropharyngeal nodes is infrequent and related to tumor location, histologic grade, and clinical stage. Lymph node involvement is more common (up to 30%) for undifferentiated and maxillary sinus carcinomas, as well as stage IV tumors. Distant metastases were infrequently seen in the past when local control of the primary tumor was uncommon; with the higher rates of local control with more modern surgical and RT techniques, more distant metastases are now being reported.
The treatment strategy for SCC, UC, and ACA depends greatly upon anatomic site and local disease extent. Surgery, when feasible, followed by postoperative RT is the treatment of choice. Invasion of surrounding structures such as dura, brain, orbit, and nasopharynx are usually considered as contraindications for surgery. For these nonoperable cases, definitive RT alone or in combination with chemotherapy is the usual approach.
A 5-year survival rate of 60% to 70% has been reported for ethmoid tumors treated by craniofacial resection and postoperative RT. Orbital exenteration may be avoided in cases of isolated bony orbital extension but it should be performed in cases of frank intraorbital involvement. With intracranial extension or involvement of the nasopharynx or base of skull, there appears to be no survival advantage for surgical debulking. In such cases, primary RT with photons results in 5-year local control rates of approximately 20%.
Surgery and postoperative RT yield the best results in early stage maxillary sinus carcinoma limited to the infrastructure with 5-year local control rates of 50% to 70% and 5- year survival figures of 40% to 65%; primary RT results in approximately 20% local control and 40% 5-year survival. Maxillary sinus tumors involving the suprastructure should be managed by aggressive surgery and postoperative RT. With this combined approach, local control rates for T3 and operable T4 tumors are 40% to 50%. Chemotherapy can be employed as neoadjuvant treatment with using a combination of different active drugs including cisplatin, 5-fluorouracil, gemcitabine, doxorubicin, methotrexate, cyclophosphamide, vincristine, and etoposide. For aggressive SCC and UC tumors, concomitant chemoradiation can be employed, typically using cisplatin and/or gemcitabine. The use of targetted therapies such as cetuximab is under evaluation in clinical studies.
Since the major oncologic risk after surgery is local relapse, postoperative RT with highly conformal techniques is recommended for most patients. Radiation doses in the postoperative setting typically range from 54 Gy to 70 Gy with conventional fractionation. Elective neck RT is often employed for T3-T4 SCC and UC. Definitive RT is adopted in cases where surgery is contraindicated using the same techniques described for postoperative RT but possibly to doses as high as 70 to 75 Gy depending on the dose to critical structures.
The use of protons for epithelial paranasal sinus tumors was studied in PROG protocol 92-15.17 All patients, >90% stage IV, were treated with hyperfractionated, accelerated proton/photon RT to a dose of 76.5 Gy. The treatment paradigm for this paranasal sinus protocol, first initiated at MGH in 1991 and supported by Loma Linda University Medical Centre (LLUMC), was concomitant boost RT to the primary tumor with protons, complementing a larger photon field incorporating both the GTV and adjuvant treatment volumes. The investigators expended significant effort to limit the total daily dose to the visual system to 180 cGy, while also respecting a total optic chiasm dose limit of 54 Gy. This often required proton treatment to a GTV volume in close (1 to 2 mm) juxtaposition to the chiasm. Dose was delivered with a mixture of photons and protons. Neuro-ophthalmologic and endocrine evaluations were performed before RT and at regular intervals during follow-up.
Primary sites were the maxillary sinus (13), ethmoid sinus (12), sphenoid sinus (3) and nasal cavity (2). The study enrolled advanced cases with a primary stage distribution of T3 in 2 cases and T4 in 23 cases. The five cases without AJCC staging were of T4-equivalent stage when classified along the guidelines for maxillary sinus and ethmoid sinus cancer. Only 4 patients had a gross total resection, with the majority having a biopsy (7) or subtotal resection (19). For the first 20 treatment days, the CTV was treated to 66 Gy (RBE) with b.i.d. fractionation. The 80% 3-year LC rate in the first 30 patients (SCC, ACC, mucoepidermoid, ACA, and sinonasal undifferentiated carcinoma) reported by Thornton in 1998 was updated by Yonemoto in 200440 reporting on the results on the first 36 patients. The 5-year local control rate was maintained in excess of 80% (including esthesioneuroblastoma subtypes) with an overall actuarial 5-year survival rate of 56%. Of particular interest was the lack of visual morbidity, despite the aggressive b.i.d. fractionation and proximity of the optic apparatus.
Reported light ion therapy series only included patients with advanced stage disease; the clinical data are still limited. Lawrence Berkeley Laboratory LBL reported on 12 patients of various histologic types treated by neon ions and noted a 5-year survival rate of 69%.19,20 The NIRS phase I study of carbon ions included ten patients (five with SCC) in whom the 5-year local control rate was 49%.21 In the phase II study, the 5-year local control was 66% (see subsequent text).29
Adenoid Cystic Carcinoma
ACC is a rare tumor, accounting for 5% to 10% of all salivary gland tumors and 1% of all head and neck malignancies. These most frequently arise from the minor salivary glands in the head and neck region and especially in the sinonasal tract. The sinonasal tract may also be invaded by lesions arising from the hard palate. ACC are characterized by having an indolent, slow-growing but often relentless, aggressive clinical course, with early perineural invasion and spread along major nerves, as well as along periosteal planes and a high rate (˜50%) of late distant metastasis to the lungs, liver, brain, and bones. On the other hand, nodal metastases are uncommon at presentation or as a late event (5%). In the MGH series, the median duration between the onset of symptoms and diagnosis of the primary tumor was 12 months. Owing to the slow-growing progression of the metastases, aggressive treatment of the primary tumor in patients with distant metastases is often warranted. ACC is considered to be relatively insensitive to chemotherapy and requires high RT doses for local tumor control. Hence, complete surgical removal of the tumor is attempted whenever possible. Adjuvant RT is generally employed as R0 resection is difficult to achieve in most paranasal sinus cancers.
Several series in the literature report the treatment results in patients with paranasal sinus ACC. Rhee et al. reported a 5-year survival figure of 85%, in spite of 5-year local recurrence and distant metastasis rates of 30% and 57% respectively (40% and 70% for T3-T4 lesions) and 10-year figures of 25% and 43% respectively.41 In patients with ACC, advanced T stage (T4), perineural invasion, major nerve involvement, omission of postoperative RT, and RT dose <60 Gy have been described as independent predictors of local recurrence.42, 43, 44 Inoperable tumors with infiltration of the skull base are considered particularly unfavorable because gross residual tumor requires high target doses rarely achievable with conventional photon RT.44,45
Proton Therapy
Twenty-four patients with newly diagnosed locally advanced ACC of skull base, unresectable or with a macroscopically incomplete resection, were treated between 1999 and 2002 at the MGH.46 A high-dose accelerated, b.i.d. fractionated photon/proton protocol was used to deliver 70 to 76.8 (mean 75.9) Gy (RBE) to the GTV or the high-risk volume. The local control rate at 5 years was 93% (two local recurrences). The main site of failure was distant metastasis (38% at 5 years). The 5-year disease-free and OS rates were 56% and 77%, respectively. In multivariate analysis, significant adverse factors predictive for survival were change in vision (p = 0.02) and sphenoid or clivus involvement (p = 0.01).
Carbon Ion Therapy
The rationale to use carbon ions in ACC paranasal tumors is based on the relatively high RBE values of up to 8 reported for high linear energy transfer (LET) RT47 and on favorable results obtained with neutrons compared with photons for unresectable or recurrent salivary gland cancers. The Radiation Therapy Oncology Group (RTOG)-Medical Research Council (MRC), randomized clinical phase III trial showed significantly better locoregional control (LRC) for fast neutron RT as compared to photon RT (56% versus 17% at 10 years).48
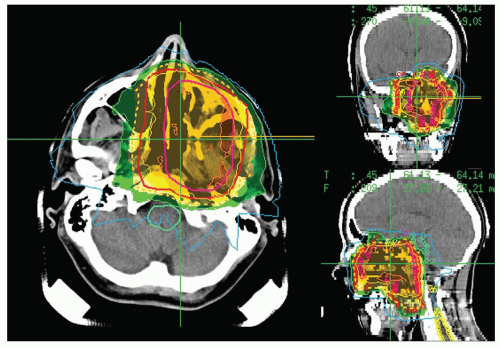
At GSI, locally advanced paranasal sinus ACC has been treated with carbon ion RT in a clinical phase I/II trial. Through September 2003, a total of 29 patients with ACC had been treated with a combination of photon IMRT to the CTV and a carbon ion boost to the macroscopic tumor. Only patients with histologically proven, inoperable, incompletely resected or recurrent ACC were included. The CTV, treated to a median dose of 54 Gy in 30 fractions of 1.8 Gy, covered the course of the involved cranial nerves up to their entry into the skull base; regional lymph nodes were not irradiated. The GTV included the macroscopic tumor with a safety margin of 1 to 2 mm. Figure 16A.4 shows a composite IMRT/carbon dose distribution. A dose of 18 Gy (RBE) carbon ion RT was delivered in six fractions of 3.0 Gy (RBE) to the GTV. With median follow-up of 16 months, the 4-year LRC and OS rates were 77% and 75.8%, respectively.49 Severe grade 4 late toxicity was observed in one patient only, who developed recurrent bacterial infections after partial resection including stabilization with metal implants and postoperative photon/carbon RT.
Similar results have been obtained with carbon ion RT at the NIRS in Japan. Between 1994 and 1997, nine patients with locally advanced ACC were treated within a dose escalation trial with carbon ions. Doses of 52.8 to 70.2 Gy (RBE) were given in 16 or 18 fractions over 4 to 6 weeks. The 5-year local control rate with carbon ion RT was 50%.21 In a phase II study of 62 patients treated with 64.0 or 57.6 Gy (RBE) in 16 fractions over 4 weeks, the 5-year local control was 74% and survival was 69%.29
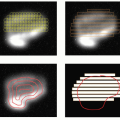
Figure 16A.4 Dose distribution (GSI, Darmstadt, Germany) for a composite plan consisting of a photon intensity-modulated radiotherapy (IMRT) component of 54 Gy and a carbon ion component of 18 Gy (RBE) in a patient with locally advanced adenoid cystic carcinoma. Maximum dose in the composite plan is 82.8 Gy (RBE), the percent isodoses relate to this maximum dose. Orange line = 90% isodose line, yellow line = 80% isodose line, green line = 50% isodose line, and blue line = 30% isodose line. The dotted yellow line represents the 60 Gy (RBE) isodose line. Dose distributions are shown in the axial, coronal, and sagittal planes.
Esthesioneuroblastoma
Olfactory neuroblastoma or esthesioneuroblastoma (ENB) is a rare tumor arising from the olfactory epithelium, representing 5% of all malignancies of the sinonasal tract.50 ENB can have variable behavior; some tumors can grow slowly whereas others are aggressive with early spread along the olfactory phyla into the anterior cranial fossa, regional cervical nodes (synchronous and metachronous node involvement has been described in >20% of patients), and distant metastases in bone, lung, pleura, liver, and the spinal epidural space. Several specific staging classifications have been proposed, including the Kadish et al.4 and the UCLA Dulguerov and Calcaterra.5 T-stage, lymph involvement, Hyams histopathologic grade, postoperative RT, and shrinkage after chemotherapy have been reported as prognostic factors for local control and survival.50, 51, 52
In a meta-analysis and review of publications between 1990 and 2000 conducted by Duguerov et al., mean values (with standard deviation [SD]) for 5-year OS and disease-free survival were 45% (22%) and 41% (21%), respectively.50 OS was different according to the treatment modalities, recognizing however that these were not randomized results and that there were low patient numbers in each treatment group. The mean (with SD) 5-year OS was 37% (33%); 48% (40%); 65% (25%); 51% (45%) and 47% (37%) respectively for RT only, surgery alone, surgery/RT, RT/chemotherapy, and surgery/RT/chemotherapy. Craniofacial resection has been associated with better local control than less extensive surgical approaches.5,53
The standard photon technique employs three fields (anterior and wedged lateral fields) with dose ranges from 55 to 65 Gy. The role of adjuvant RT after surgery has been reported in several series.52 The role of cervical RT in N0 patients is still a matter of debate.54 The use of neoadjuvant and adjuvant chemotherapy has also been advocated for this pathology.
Proton Therapy
The role of protons for ENB has been assessed by the MGH group. The treatment schedule was first published in 1997:55 two cycles of cisplatinum and etoposide chemotherapy, followed for responders by combined photon/proton RT of 68 Gy (RBE) to the primary site, or for poor responders by surgical resection followed by RT. In both cases, two additional cycles of adjuvant chemotherapy were added. The b.i.d. RT protocol was based on the same concomitant irradiation strategy as was employed for the more common sinus histologies (1.8 Gy photons in the AM + 1.5 Gy [RBE] protons in the PM), albeit to a lower cumulative dose. Fitzek et al. published the results of 19 patients so treated from 1992 to 1998 (pure ENB in 10 and neuroendocrine or mixed tumors in 9).56 Seventy-nine percent of the patients had Kadish stage C tumors and 74% had base of skull involvement. The median dose to the macroscopic tumor ranged from 67.2 to 72.6 (median 69.2) Gy (RBE) in 38 to 43 (median 40) fractions (range 38-43) over 29 to 49 (median 38) days. The proton component was variable because of scheduling constraints at the HCL—the median proton dose was 22.8 Gy (RBE) until 1996; thereafter it was 43.1 Gy (RBE). The neck was irradiated in all patients (45 Gy in 1.8 Gy/fraction, 5 days a week with photons).56 With a median follow-up of 45 months (range, 20-92), the actuarial 5-year survival, progression-free survival and local control were 74% (SD 48% to 99%), 78.9% (SD 54% to 94%) and 88% (SD 68% to 99%), respectively. Four patients died of metastases (liver, bone, meninges, and spine). Two patients experienced local failure, both salvaged with surgery. The 5-year local control rate with the initial treatment was 88% and was 100% with surgical salvage. Four patients developed frontal/temporal lobe damage; this was grade 2 in three patients who received short-term steroid treatment and grade 3 in one patient. This series was updated in 2004, and included 34 patients at that time.16 With 45 months’ mean follow-up, local control at 3 years was 91%. The principal cause of failure was metastatic disease.
Preliminary data from 13 patients treated with protons ± surgery in Kashiwa, Japan were recently presented.18 The dose was 65 Gy (RBE) in 26 fractions over 6 to 7 weeks. With a median follow-up of 24 months (range 2 to 53), 3-year local control and OS rates were 71% and 90%, respectively. Regional lymph nodes metastases developed in one patient whereas distant metastasis was noted in another.
Mucosal Melanoma
Mucosal melanoma (MM) of the paranasal sinuses and nasal cavity is rare, representing <2% of all melanoma cases and approximately 3% to 4% of all sinonasal tumors; nevertheless, it is the most common site of melanoma in the respiratory tract. The most common anatomic sites of involvement are the nasal septum, turbinates, lateral wall of the nasal fossae, and maxillary and ethmoid sinuses.57
Angioinvasiveness appears to predispose to metastases. Advanced disease stage, tumor invasion deeper than 5 to 7 mm, and multicentricity are also associated with a worse prognosis. Amelanotic lesions seem to have a worse prognosis whereas tumors arising on melanotic macules can be less aggressive.
Surgery is the standard treatment of MM of the upper aerodigestive tract. Patients undergoing radical surgical resection fare better than those treated with nonradical surgery or nonoperatively.58 Resection should be performed with wide excision of the primary tumor and regional lymph node dissection when node-positive. Postoperative RT is recommended for macroscopic or microscopic residual disease or as a definitive treatment when surgery is not feasible;59, 60, 61 in this latter situation, consideration should also be given to adding systemic therapy. While large doses per fraction (>4 Gy) have been advocated by some to overcome the relative radioresistance of melanoma cells, there is no documented clinical advantage to date for hypofractionation for MM.58
High-LET particles for MM can be justified by the relative radioresistance of some melanoma cells as demonstrated by in vitro studies that show a broad shoulder on survival curves in some melanoma cell lines.62 Neutrons were tested in skin and mucosal melanoma with quite favorable results at Hammersmith Hospital.63 More recently a series of 76 cases of mucosal melanoma, 61 of them (80%) from the paranasal sinus and nasal cavity, was reported from NIRS.22 No patient underwent surgical resection. Carbon ion therapy was performed to a total dose of 57.6-64.0 Gy (RBE) in fractions of 3.6 to 4.0 Gy (RBE). The local control results from the whole series were very encouraging with a 5-year local control rate of 77%; 5-year OS, however, was only 26% due to the very high incidence of distant metastases. This prompted a phase II study of carbon ion RT for malignant melanoma (44 cases) with concomitant chemotherapy consisting of DAV—day 1: DTIC (dacarbazine) 120 mg/m2, ACNU (1-(4-amino-2-methyl-5-pyrimidinyl)-methyl-(2-chloroethyl)-3-nitrosourea) 70 mg/m2, and vincristine 0.7 mg/m2; days 2 to 5: DTIC 120 mg/m2. Cycles were given at 4-week intervals for five courses. The 4-year local control and survival rates were 85% and 44%, respectively. When the GTV was <50 mL, the 4-year survival was 62%.29 These data show carbon ions are very effective in obtaining local tumor control. Further investigational studies with systemic therapy are needed to improve long-term survival.
Only gold members can continue reading. Log In or Register to continue