CHD has an incidence of approximately 8 per 1000 live births; the 10 most common entities account for 80% of all cases (Table 1.74).
Historically, the conventional chest radiograph has played a significant role in the work-up of children with CHD. There have been numerous descriptions that were so-called diagnostic for CHD; one could think of the “egg on string” sign in case of transposition of the great vessels. However, as the presentation of CHD on the chest radiograph depends on a multitude of factors, these signs are not diagnostic (for completeness, we will present them in the tables of this chapter).
A study in 128 children with suspected CHD showed that conventional chest radiograph has a sensitivity of 26%–59% for structural heart disease and an equally poor positive predictive value of 46%–52%. It is important to note that there is no evidence that conventional radiographs can serve as a screening test for CHD.
Currently, the most widely adopted diagnostic strategy is primary imaging with cardiac US. Based on the US findings, either CT, if anatomy needs to be depicted, or MRI, if functional imaging or depiction of intracardiac anatomy is needed, will be performed. Diagnostic angiography is now rarely performed and only in those cases where CT and/or MRI are not diagnostic or if pressure measurements are necessary.
It is also important to note that cardiac imaging is a “team sport” in which a close collaboration between the cardiologists and radiologists is essential.
Table 1.74 Incidence of top 10 CHD
Condition
Incidence (%)
Cyanotic CHD
Transposition of great vessels
Tetralogy of Fallot
4
4
Obstructive CHD
Pulmonary stenosis
Aortic stenosis
Coarctation
Hypoplastic left heart syndrome
9
5
5
4
CHD with left-to-right shunt
Ventricular septal defect
Patent ductus arteriosus
Atrial septal defect
Arterioventricular septal defect
36
9
5
4
Table 1.75 Dynamically increased pulmonary vascularity (left-to-right shunt) without cyanosis
In case of a small defect, the cardiac silhouette and vessels have a normal appearance. If the defect is large they enlarge. With a large defect and high right ventricular and pulmonary pressure (Eisenmenger syndrome), the hilar vessels become enlarged and in contrast the lung markings become diminished towards the periphery.
Twenty-five percent of all congenital cardiac anomalies. Clinical symptoms are dependent on the size of the VSD.
Cardiomegaly and prominent pulmonary artery. On the lateral chest radiograph an increased contact area between the sternum and the heart is seen (infundibular expansion).
In the neonatal period, the lung fields may become dense over time due to pulmonary edema. Cardiomegaly and increased pulmonary flow may occur in infants.
In neonates, the Botallian duct may remain patent or reopen.
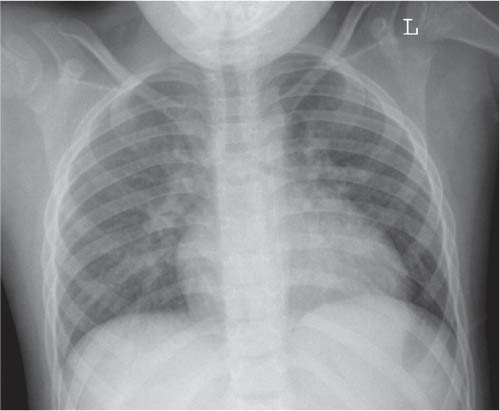
Fig. 1.201 Chest radiograph with increased vascular markings in a 5-year-old girl.Fig. 1.202 Anteroposterior chest radiograph of a 16-month-old boy with ASD.Fig. 1.203 PDA. Chest radiograph in a premature neonate with increased vascular markings and a large cardiac shadow indicative of a persistent Botallian duct.
Table 1.76 Dynamically increased pulmonary vascularity with cyanosis
Enlarged cardiac silhouette where the heart is oval in shape and the cardiac apex is upturned. There is a narrow vascular pedicle (slender mediastinum). Classic sign: “egg-on-a-string.”
The systemic and pulmonary circulations are transposed and therefore separated; an ASD or VSD is obligatory for survival.
Type I: Origin of a single pulmonary trunk from the left lateral aspect of the common arterial trunk, with branching of the left and right pulmonary arteries from the pulmonary trunk.
Type II: Separate but proximal origins of the left and right pulmonary arterial branches from the postero-lateral aspect of the common arterial trunk.
Type III: Branch pulmonary arteries originate independently from the common arterial trunk or aortic arch, most often from the left and right lateral aspects of the trunk.
AVSD: endocardial cushion defect, septum primum defect, ASD I
Cardiomegaly with mild increase of pulmonary vascularity.
Common in trisomy 21.
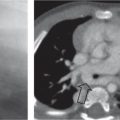
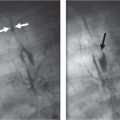
Fig. 1.204 a–c Pulmonary venous drainage. (a) Type III TAPVR in a 1-month-old boy shows increased vascularity in the right lung. The draining vein is not visible. (b) Radiograph of the same patient after closure of the aberrant pulmonary vein, at the age of 5 months, using an amplatzer device (arrow). (c) Posteroanterior chest radiograph of a 14-year-old boy with CGD wearing a scimitar on a necklace.Fig. 1.205 Classic “egg-on-a-string” sign in a 1-day-old boy.Fig. 1.206 Schematic representation of truncus arteriosus.Fig. 1.207 AVSD in a 6-week-old girl with Down syndrome. Note the cardiomegaly and increased vascularity.
Diffuse bilateral opacification of the lungs; the heart initially has a normal size but may enlarge later in life.
The imaging findings mimic pneumonia and overhydration.
Table 1.78 Congenital cardiac anomalies with decreased pulmonary vascular markings (flow): obstruction at the level of the right heart, with right-to-left shunting and cyanosis
As a result of decreased pulmonary vascularity, the lungs are hyperlucent. The cardiac silhouette is normally not enlarged. The heart may assume a “boot” shape (coeur en sabot).
Right-sided aortic arch in 25% of cases.
Tetralogy of Fallot consists of pulmonary stenosis, right ventricular hypertrophy, VSD, and overriding aorta.
Pulmonary valve anomaly
Poststenotic dilatation of the pulmonary outflow tract.
Significant cardiomegaly in combination with a slender vascular pedicle.
In most cases, a right-to-left shunt with cyanosis is present.
Fig. 1.208 Chest radiograph of a 5-week-old boy with tetralogy of Fallot. Note the uplifted apex leading to a boot-shaped heart.Fig. 1.209 A 1-day-old boy with Ebstein anomaly.
Cardiac Positional Anomalies
On chest radiographs, the position of the heart can be defined as dextrocardia, mesocardia, and levocardia. However, as the position of the heart is defined by the position of the atria, where the right atrium lies on the right side and the left atrium on the left side, plain radiographs cannot rule out positional anomalies in all cases. For this, cardiac US is the diagnostic modality of choice.
The tracheobronchial tree morphology is, in general, in keeping with the position of the atria and thus can serve as a guide in deciding the cardiac situs on chest radiographs.
Table 1.79 Cardiac positional anomalies
Diagnosis
Findings
Comments
Levocardia
Physiologi
Normal anatomic position of the heart.
Isolated
The heart is left-sided, but there is an abdominal situs inversus.
Often in combination with congenital cardiac anomalies.
Kartagener syndrome (also known as immotile cilia syndrome); combination of situs inversus totalis, bronchiectasia, and chronic sinusitis.
Ivemark syndrome
Dextroisomerism in which both lungs have three lobes and an epiarterial bronchus. There is asplenia and in up to 33% of cases there is dextrocardia.
Commonly associated with severe congenital cyanotic heart disease.
Isomerism
Isomerism
Midline position of the heart, liver, and stomach. Both sides of the body may have a more or less left-or right-sided morphologic layout.
Commonly associated with CHD.
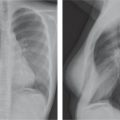
Fig. 1.210 Isolated dextrocardia in an 8-year-old boy. Note the position of the NG tube in the normally positioned stomach (arrow).Fig. 1.211 Situs inversus totalis in a 21-month-old girl. Note the right-sided gas bubble in the stomach (asterisk).Fig. 1.212a, b Situs inversus totalis. (a) Watersview of a male teenager showing opacification of the the maxillary sinus, in keeping with sinusitis. (b) Posteranterior chest radiograph of the same patient as in (a) shows dextrocardia. The diagnosis Karthagener syndrome was made.
Only gold members can continue reading. Log In or Register to continue