Diaphragmatic eversion and contralateral mediastinal displacement.
Requires emergency needle thoracotomy.
Hydropneumothorax
Air-fluid level with horizontal interface on horizontal beam film.
Pseudopneumothorax
Most commonly due to overlying skin fold. No pleural line visible. Interface between densities may fade out or extend beyond the chest wall.
Repeat film with corrected rotation may be required.
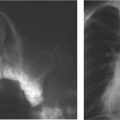
Fig. 1.75 Subpulmonary pneumothorax. Chest radiograph in an 18-month-old boy following surgery for pulmonary atresia. There is a lucency below the right lung whose lower margin is crisply defined (arrows). This is not drained by the apically placed pleural drain.Fig. 1.76 Anteromedial pneumothorax. Chest radiograph in a 5-month-old child following cardiac surgery. There is a medial lucency on the left with crisp definition of the heart border. The medial lung edge is visualized (black arrow). There is deepening of the left costophrenic sulcus (white arrow).
Table 1.37 Pneumothorax cases
Diagnosis
Findings
Comments
Barotrauma
Often preceded by or coexisting with pulmonary interstitial emphysema.
Common in ventilated neonates, particularly those with HMD and meconium aspiration syndrome. Hypoplastic lungs are also prone to barotrauma.
Trauma
Iatrogenic, penetrating injury, blunt trauma to chest.
Evidence of underlying disease (e.g., peribronchial thickening). Blebs/bullae rarely visualized.
Particularly CF and asthma: rupture of blebs and bullae, or overdistended acini in areas of air trapping. In CF, lung may not collapse completely owing to reduced compliance.
Infection
Cavitating pneumonia occasionally spreads to pleural space. Often complicated by bronchopleural fistula.
Particularly with TB.
Interstitial lung disease
Evidence of underlying disease. Usually cystic change or established fibrosis present.
In children, LCH is the most common interstitial lung disease to cause pneumothorax.
Malignant disease
Subpleural pulmonary metastases.
Usually sarcoma, particularly osteosarcoma.
Spontaneous
Normal underlying lungs: very occasionally visualize bleb.
Rare in young children. Typically in tall athletic males. Occasionally in Marfan syndrome.
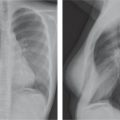
Fig. 1.77 Pneumothorax in cystic fibrosis. Chest radiograph in a 15-year-old with known CF and chest pain. There is a small left-sided pneumothorax; the lung edge and pleura clearly visible (arrows). The lung does not collapse owing to reduced compliance.
Diaphragm appears to be peaked laterally. US used to confirm.
Pseudoeffusion
Usually due to skin fold from overlying arm.
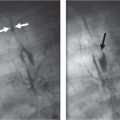
Fig. 1.78a, b Subpulmonic effusion. (a) Chest radiograph in a 3-dayold boy with congenital heart disease. The right hemidiaphragm appears elevated and flattened (black arrow). There is pleural fluid laterally (white arrows). (b) Coronal US image in the same patient. There is a large predominantly subpulmonary effusion. The white arrow indicates the diaphragm, and the open arrow indicates the lung.
Table 1.39 Pleural effusion causes
Diagnosis
Findings
Comments
Parapneumonic
Underlying lung consolidation. US may show minor septation or simple anechoic effusion.
Distinction from empyema frequently requires aspiration.
Difficult to distinguish from simple parapneumonic effusion on radiograph. May be lobulated.
US: echoic fluid, thin or thick septations or even solid appearing collection.
CT: pleural enhancement, thickening of extrapleural fat, lobulated appearing collection.
Commonly following streptococcal or staphylococcal pneumonia. Incidence may be rising in children. Treated with either tube thoracostomy with fibrinolytics or surgically (usually video-assisted thoracoscopy).
Tuberculous
Primary complex often not visible.
Rare prior to school age. Ten percent of primary TB.
Neoplastic
CXR: may visualize lobulated pleural mass.
CT: irregular/nodular pleural thickening.
Common causes: leukemia/lymphoma. Metastatic disease particularly Wilms tumor, and sarcoma, primary tumors including PNET, Askin disease, mesothelioma.
Fluid milky after feeding. May be idiopathic, secondary to lymphatic injury (e.g., birth trauma, cardiac surgery), or associated with lymphangiectasia.
Pancreatitis
Usually left-sided and small.
Subphrenic abscess
Usually small, sympathetic effusion.
Transudative
Often larger on the right.
In low albumin states, cardiac failure, “third spacing” in sepsis.
Hemothorax
Hyperdense on CT examination: density measures 30–80 Hounsfield units (HU) depending on age of blood.
Usually following trauma or iatrogenic.
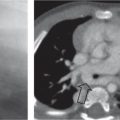
Fig. 1.79 Empyema. Axial contrast-enhanced CT image in a 3-year-old boy with empyema referred for surgical drainage. There is an irregular left pleural collection with pleural thickening and enhancement and widening of the subcostal fat space (black arrow). The underlying lung demonstrates an area of cavitary necrosis (white arrows), which has a recognized association with empyema.Fig. 1.80 Neonatal chylous pleural effusion. Thoracoabdominal radiograph in a neonate. There is a large left-sided pleural effusion (black arrow) and a smaller right-sided effusion (white arrows). Fluid was chylous on aspiration.
Leukemia, neuroblastoma, and Wilms tumor most common primary lesions.
Ipsilateral pulmonary vascular anomaly
Pleural companion shadows due to collateral vessels in pleural space. Occurs in pulmonary artery or vein atresia.
Primary pleural neoplasm
Lipoma: fat density areas.
Liposarcoma: nonspecific infiltrative mass.
Mesothelioma: Not asbestos-related: occasionally following radiotherapy. Similar to adult form.
All rare.
Fig. 1.81 Pleural thickening following empyema. Chest radio-graph in an 18-month-old girl 1 month following tube thoracostomy for empyema. There is residual irregular pleural thickening (arrows).Fig. 1.82a, b Pleural metastasis. (a) Chest radiograph in a 5-year-old girl with previous stage 4 Wilms tumor: note lung sutures in right lung from previous nodule resection (open arrow). There is an ill-defined mass in the left lower zone with a broad diaphragmatic pleural base (black arrow) and some lobulated lateral pleural thickening (white arrow). (b) Coronally reformatted CT image in the same patient confirms presence of large pleurally based mass in left costophrenic angle: biopsy confirmed relapsed Wilms tumor.
Diaphragmatic Defects
Table 1.41 Diaphragmatic hernias and congenital diaphragmatic defects
More commonly left-sided. Usually contains bowel ± solid viscera. NG tube and umbilical catheters may deviate toward defect. Gas in hernia in continuity with abdominal bowel gas, which is sparse. Compresses ipsi-lateral ± contralateral lung, resulting in hypoplasia.
Large defects almost invariably presenting in neonatal period.
Predominantly right-sided (10:1). Hepatic lobe (s), stomach, duodenum, small and large bowel, as well as spleen and omentum may all herniate. Chest and abdomen radiograph: soft-tissue density projected over the costophrenic and cardiophrenic angles. Lateral view: only the posterior portion of the diaphragm is discernable, the hernia is retrosternal density. The plain radiograph is often sufficient, especially when the hernia contains aerated bowel. US, possibly CT. Scintigraphy if hemorrhaging.
Rare approximately 7% of congenital hernias; very rarely bilateral. Early childhood, adulthood. Associated anomalies: scimitar syndrome, unilobar lungs, Hirschsprung disease. Complications: incarceration, gastric volvulus. Many are asymptomatic.
More commonly right sided. Diaphragm shows reduced excursion and lobulated contour with upward displacement.
Due to a congenitally thin diaphragm. Unilateral associated with trisomies 13, 15, and 18, and Beckwith-Wiedemann syndrome. Bilateral in congenital CMV infection and toxoplasmosis.
Hiatus hernia
Widening of the esophageal hiatus. Central supradiaphragmatic hernia, mainly consisting of a small section of the cardia, varying from a small nubbin to several centimeters. Lateral view: middle mediastinum. Sliding hernia seen only in inspiration. Gastroesophageal overdistention may be required to demonstrate gastroesophageal reflux. Danger of reflux esophagitis, even peptic esophageal stricture. US, endoscopy.
Gastroesophageal reflux and vomiting from birth, failure to thrive, iron deficiency anemia, melena, and hematemesis indicate reflux esophagitis. Infants are most commonly affected.
Cardia in normal position part of stomach herniates alongside the esophagus through the esophageal hiatus. Right more common than left. Plain radiograph: circular “cyst” in the cardiophrenic angle. Lateral view: central in position. Confirmation with a contrast study.
Mainly in older infants and school age children. Seldom symptoms, occasionally vomiting.
Bochdalek hernia (lumbocostal and pleuroperitoneal canals)
Predominantly left-sided. Herniation of stomach, spleen, and bowel; liver when right-sided. Kidney position high. The hemithorax is initially dense after birth, becoming cystic or honeycombed when the bowel fills with air. The diaphragm is not identified. Mediastinum deviated to the contralateral side. Small scaphoid abdomen with no air, absent liver shadow. US (prenatal and postnatal).
Most common true diaphragmatic defect, rarely with a hernial sac. Severe illness. Decisive for the prognosis: degree of ipsilateral and contralateral pulmonary hypoplasia. Commonly associated with other anomalies (cardiovascular, malrotation, skeletal, etc). Requires immediate surgical repair and/or ECMO until the lungs mature. Prognosis: still only 45% survival rate.
Bochdalek hernia: less severe forms, diagnosed later
Left more common than right. Dense homogeneous or cystic honeycombing appearance caused by air-containing bowel loops. Lateral view posterolateral herniation.
In neonates or in older infants. Milder clinical symptoms than with the larger defect, occasionally even an incidental finding. Associated with other anomalies.
Bochdalek hernia: late type, delayed presentation
Radiographic findings only after the first or second week of life, occasionally even later. Initially normal chest radiograph, with sudden onset of density and mediastinal shift. When right-sided: “absent liver” sign, as the liver is displaced into the thorax, and air-containing bowel loops fill the right upper quadrant of the abdomen.
Origin is unclear; it is thought that the liver and spleen prevent hermiation in infancy. Clinical symptoms occur simultaneously with the radiographic changes.
Fig. 1.83 Bochdalek hernia. Chest radiograph in a neonate with antenatally diagnosed diaphragmatic hernia. There are bowel loops within the left hemithorax, including the stomach which contains an NG tube (arrow).Fig. 1.84a, b Morgagni hernia. (a) Chest radiograph in an infant with antenatally diagnosed diaphragmatic defect. There is a soft-tissue–dense opacity in the right medial lower zone (arrows) obscuring the right heart border. (b) Lateral screen grab image from fluoroscopic examination of the same child following barium administration via NG tube. A loop of bowel herniates into the chest via an anterior diaphragmatic defect (arrow).Fig. 1.85a, b Morgagni hernia. (a) Chest radiograph shows a Morgagni hernia. (b) US of the same patient shows herniation of the left liver lobe.Fig. 1.86a, b Diaphragmatic eventration. (a) Chest radiograph in an 11-month-old boy with the VATER association (v ertebral anomalies, a nal atresia, t racheoesophageal fistula, e sophagel atresia, r enal and/or r adial anomalies). There is a focal bulge to the left hemidiaphragm (arrows). (b) Lateral chest radiograph in the same child confirms focal diaphragmatic bulging in the midportion, containing some bowel gas within (arrows).Fig. 1.87 Barium follow-through of a paraesophageal hernia with jejunal involvement in a 2-month-old girl.Fig. 1.88a, b Bochdalek hernia. (a) Bochdalek hernia in an 8-year-old boy. (b) CT of the same patient shows the posterior paravertebral location of the herniation.Fig. 1.89 Left-sided diaphragmatic hernia.Fig. 1.90 Right-sided diaphragmatic hernia.Fig. 1.91a, b Left-sided diaphragmatic hernia. (a) Left-sided diaphragmatic hernia with an intrathoracic stomach. (b) CT of the same patient shows a dilated intrathoracic stomach.
Only gold members can continue reading. Log In or Register to continue