Liver, biliary, and splenic scintigraphy have played an important diagnostic imaging role in patient management since the 1960s. Today’s radiopharmaceuticals have mechanisms of uptake and localization that take advantage of the complex anatomy and physiology of the liver ( Table 9.1 ; Figs. 9.1 to 9.4 ). Although many of the radiopharmaceuticals, methodologies, and indications have changed, hepatobiliary and splenic scintigraphy continue to provide unique functional diagnostic information not available from anatomical imaging such as computed tomography (CT) or ultrasonography.
| Radiopharmaceutical | Mechanism of Uptake | Indication |
|---|---|---|
| Tc-99m mebrofenin, disofenin | Hepatocyte | Cholescintigraphy |
| Tc-99m red blood cells | Blood-pool distribution | Hemangioma, splenosis |
| Tc-99m sulfur colloid | Kupffer cell | Focal nodular hyperplasia, splenosis, liver function |
| Tc-99m MAA | Blood flow, capillary occlusion | Hepatic arterial perfusion |
| Y-90 microspheres | Blood flow, capillary occlusion | Hepatic arterial tumor therapy |
| F-18 FDG | Glucose metabolism | Tumor/infection imaging |
| Gallium-67 citrate | Iron binding | Tumor/infection imaging |




Cholescintigraphy
Cholescintigraphy is ordered by physicians and surgeons for the diagnosis of a variety of acute and chronic hepatobiliary diseases, including acute cholecystitis, biliary obstruction, biliary leak, and chronic acalculous gallbladder disease ( Box 9.1 ).
Acute cholecystitis
Acute acalculous cholecystitis
Chronic cholecystitis
Chronic acalculous gallbladder disease
Biliary obstruction
Biliary atresia
Sphincter of Oddi dysfunction
Biliary leak
Biliary diversion assessment
Biliary stent function
Focal nodular hyperplasia
Enterogastric bile reflux
Radiopharmaceuticals
Three Tc-99m-labeled hepatobiliary radiopharmaceuticals have been approved by the Food and Drug Administration (FDA) for clinical use (see Fig. 9.4 ). The first, Tc-99m dimethyl iminodiacetic acid (Lidofenin or hepatic iminodiacetic acid [HIDA]), is no longer used because of its poor uptake in patients with hepatic dysfunction. The term HIDA is now commonly used to describe all Tc-99m hepatobiliary radiopharmaceuticals. The two presently in clinical use in the United States are Tc-99m disofenin (Hepatolite) and Tc-99m mebrofenin (Choletec; Table 9.2 ).
| Chemical Name | FDA Name | Commercial Name |
|---|---|---|
| Tc-99m diisopropyl IDA (DISIDA) | Disofenin | Hepatolite |
| Tc-99m bromotriethyl IDA | Mebrofenin | Choletec |
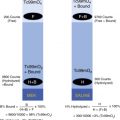
For these hepatobiliary radiopharmaceuticals, Tc-99m serves as a bridging atom between two iminodiacetic acid (IDA) ligand molecules, both of which bind to a lidocaine analog that determines the radiopharmaceutical’s biologic and pharmacokinetic properties (see Fig. 9.4 ). Minor structural changes in the phenyl ring (N substitutions) result in significant alterations in the pharmacokinetics of IDA radiopharmaceuticals ( Table 9.3 ). Numerous Tc-99m HIDA analogs have been investigated; however, all had less uptake and slower clearance than the two currently approved radiopharmaceuticals ( Fig. 9.5 ).
| Radiopharmaceutical | Hepatic Uptake (%) | Biliary Clearance Half-Time (min) | 2-hr Renal Excretion |
|---|---|---|---|
| Tc-99m disofenin (Hepatolite) | 88 | 19 | <9% |
| Tc-99m mebrofenin (Choletec) | 98 | 17 | <1% |

After intravenous injection, Tc-99m HIDA radiopharmaceuticals are tightly bound to protein in the blood, thus minimizing renal clearance. They are organic anions extracted and excreted by the liver in a manner similar to bilirubin and bile. Unlike bilirubin, Tc-99m HIDA radiopharmaceuticals are excreted in their original radiochemical form without conjugation or metabolism. Because Tc-99m HIDA travels the same pathway as bilirubin, it is subject to competitive inhibition by elevated serum bilirubin levels. The radiotracer enters the gallbladder via the cystic duct and the second portion of the duodenum via the common bile duct ( Fig. 9.6 ; see also Fig. 9.2 ). Distribution between the gallbladder and biliary ducts varies depending on the patency of the ducts, sphincter of Oddi tone, and intraluminal pressures. The gallbladder normally begins to fill before biliary-to-bowel transit.


Hepatic dysfunction results in altered HIDA pharmacokinetics—delayed uptake, secretion, and clearance ( Figs. 9.7 and 9.8 ). Therefore, the normal time of gallbladder filling and biliary-to-bowel clearance may be delayed. The kidneys serve as the alternative route of excretion. Although only a small percentage of the dose is normally cleared by this path, urinary excretion increases with hepatic dysfunction. Because of high radiopharmaceutical extraction efficiency, diagnostic images can be obtained in patients with bilirubin levels of 20 to 30 mg/dL, although image quality lessens. Mebrofenin has greater hepatic extraction and resistance to displacement by bilirubin than disofenin does; thus, it is preferred in patients with poor liver function. Radiation dosimetry is detailed in the Appendix.




Patient Preparation
Patients must ingest nothing by mouth for 3 to 4 hours before the study because food stimulates the endogenous release of cholecystokinin (CCK) from the proximal small bowel, resulting in gallbladder contraction and thus potentially preventing radiotracer entry. On the other hand, if the patient has been fasting for > 24 hours, the gallbladder has no stimulus to contract and thus will likely contain viscous bile, which can also prevent radiotracer entry. In this situation, the patient should be administered sincalide (Kinevac, CCK) before the clinical study to empty the gallbladder. Tc-99m HIDA should be administered at least 30 minutes after the completion of sincalide infusion to allow sufficient time for gallbladder relaxation. All opiate drugs should be withheld for at least 6 hours or three half-lives before radiopharmaceutical injection. Opiates contract the sphincter of Oddi, potentially producing a picture of functional partial biliary obstruction, indistinguishable from a true obstruction.
Pertinent patient history before starting the study includes the following: What is the clinical question being asked by the referring physician? Are the symptoms acute or chronic? Has sonography or other imaging been performed, and what were the results? Has the patient had biliary surgery? If the patient had a biliary diversion procedure, what is the anatomy? Are there intraabdominal tubes or drains? If so, where are they placed, and which tubing drains each? Should the drains be open or clamped to answer the clinical question? Did the patient’s most recent meal contain sufficient fat (10 g) to contract the gallbladder?
Methodology
A protocol for cholescintigraphy is detailed ( Box 9.2 ). Acquisition of 1-minute frames for 60 minutes is standard. An initial 60-second flow study is optional (1–3 seconds/frame) but can occasionally add useful information. At 60 minutes, right lateral and left anterior oblique views should be performed to confirm or exclude gallbladder filling, which at times may be uncertain due to bile in the biliary ducts and duodenum overlapping the gallbladder fossa. Delayed imaging, morphine sulfate, and CCK are options for specific clinical indications.
Patient Preparation
Nothing by mouth for 4 hours before the study.
If the patient is fasting for >24 hours, infuse sincalide 0.02 μg/kg over 60 minutes. Wait at least 30 minutes after sincalide infusion is complete before infusing the radiopharmaceutical.
Hold all opiate drugs for at least 6 hours.
Radiopharmaceutical
Tc-99m Mebrofenin—Intravenous Injection
| Bilirubin | Dose | |
|---|---|---|
| Adults | ||
| <2 mg/dL | 5.0 mCi (185 MBq) | |
| 2–10 mg/dL | 7.5 mCi (278 MBq) | |
| >10 mg/dL | 10.0 mCi (370 MBq) | |
| Children | ||
| 0.05 mCi/kg (1.85 MBq/kg) | Minimum dose 0.5 mCi (18.5 MBq) | |
Instrumentation
Camera: Large-field-of-view gamma camera
Collimator: Low-energy parallel hole—high resolution
Window: 15% to 20% over 140-keV photopeak
Patient Positioning
Supine; field of view should include upper abdomen.
Computer Setup
1-second frames × 60 for flow study, then 1-minute frames × 59
Imaging Protocol
- 1.
Start computer, then inject Tc-99m mebrofenin intravenously.
- 2.
At 60 minutes, acquire right lateral and left anterior oblique images.
- 3.
If acute cholecystitis is suspected and the gallbladder has not filled, inject morphine sulfate (or) obtain delayed images up to 3 to 4 hours.
- A.
If liver activity has washed out, reinject half-dose Tc-99m mebrofenin before morphine infusion.
- B.
Morphine infusion: If good biliary duct clearance and biliary-to-bowel transit, inject intravenously 0.04 mg/kg over 1 minute. Acquire 1-minute frames for 30 minutes.
- C.
As alternative to morphine for poor biliary duct clearance (<50%) and poor biliary-to-bowel transit, obtain delayed images at 2 and 4 hours.
- A.
- 4.
If suspected partial biliary obstruction (delayed biliary duct clearance and biliary-to-bowel transit) at 60 minutes, administer sincalide over 60 minutes or obtain delayed 2- and 4-hour images.
- 5.
Delayed imaging is also indicated in the setting of hepatic insufficiency or suspected slow leak.
Cholescintigraphic Diagnostic Patterns
Blood Flow
During the arterial flow phase, the spleen and kidneys are first seen (see Fig. 9.6 ). The liver appears during the venous phase because of its predominantly portal blood flow (75% portal vein, 25% hepatic artery). Early hepatic flow may be seen with arterialization of the liver’s blood supply (e.g., in cirrhosis or generalized tumor involvement; see Fig. 9.7 ). With severe acute cholecystitis, there may be increased flow to the gallbladder fossa ( Fig. 9.9 ). Focal increased flow may also be seen with intrahepatic abscess, malignant mass, and focal nodular hyperplasia.

Hepatic Uptake and Function
Liver function is best judged by noting how rapidly the cardiac blood pool clears. With good hepatic function, it clears within 5 to 10 minutes (see Fig. 9.6 ). With hepatic dysfunction, there is delayed clearance (see Figs. 9.7 and 9.8 ). During the early hepatic uptake phase, liver size can be approximated and intrahepatic lesions noted. Most intrahepatic masses will have decreased uptake compared with adjacent liver, except for focal nodular hyperplasia.
Gallbladder Filling
The normal gallbladder begins to fill by 10 minutes and is usually well seen by 30 to 40 minutes (see Fig. 9.6 ). Visualization beyond 60 minutes is considered delayed ( Fig. 9.10 ). Right lateral and left anterior oblique views can help confirm or exclude gallbladder filling ( Fig. 9.11 ). In the right lateral projection, the gallbladder is anterior and to the viewer’s right. In the left anterior oblique view, the gallbladder, an anterior structure, moves toward the patient’s right; the common duct and duodenum, more posterior structures, move to the patient’s left. Upright imaging and ingestion of water can be used to clear duodenal activity when needed.


Biliary Clearance
Duct size is not well assessed with cholescintigraphy. The smaller peripheral biliary ducts are seen. The larger left and right hepatic bile ducts, common hepatic duct, and common bile duct are typically seen. Prominent ducts do not necessarily signify obstruction. The left hepatic ducts sometimes appear more prominent than the right because of the anterior position of the left lobe and close proximity to the gamma camera. The strength of scintigraphy is to confirm or exclude duct patency, not to diagnose dilatation. The common bile duct is normally seen by 20 minutes. By 60 minutes, ductal activity decreases by > 50% of peak activity, and clearance into the small bowel is seen.
Pharmacological Interventions Before or During Cholescintigraphy
Morphine Sulfate
Morphine sulfate (MS) can be used as an alternative to 3- to 4-hour delayed imaging in patients with nonfilling of the gallbladder referred for suspected acute cholecystitis. If the gallbladder has not visualized by 60 minutes, low-dose morphine (0.04 mg/kg) is infused intravenously, producing contraction of the sphincter of Oddi, thus increasing intrabiliary pressure, resulting in preferential filling of the gallbladder, if the cystic duct is patent ( Fig. 9.12 ). The answer to filling or nonfilling of the gallbladder is known by 30 minutes. Some clinics give morphine at 30 minutes if bowel activity is seen. Be aware that morphine may inhibit the effect of subsequently administered cholecystokinin.

Cholecystokinin
CCK is a polypeptide hormone released by mucosal cells in the proximal small bowel in response to ingested fat and protein. The terminal octapeptide of CCK is the physiologically active portion of the hormone ( Fig. 9.13 ). Binding of CCK with receptors in the gallbladder wall and sphincter of Oddi results in gallbladder contraction and sphincter relaxation. Bile is then discharged into the small intestines, where it facilitates intestinal fat absorption. Sincalide (Kinevac), an analog of the terminal octapeptide of CCK, is the commercial form of CCK. In patients who have not eaten within 24 hours, it should be administered before the study to empty the gallbladder. Tc-99m HIDA should not be injected until at least 30 minutes after the conclusion of sincalide infusion, to allow time for gallbladder relaxation so that the radiotracer can enter.

Imaging Gallbladder Contraction
Fatty meals and CCK have been used to evaluate gallbladder contraction. An underlying assumption is that gastric emptying is normal. Delayed gastric emptying results in delayed endogenous stimulation of CCK from the proximal small bowel and thus potentially delayed and reduced gallbladder contraction during the standard imaging time. Alternative cholecystogogues have been used and normal values established (e.g., whole milk, EnsurePlus, and corn oil emulsion). However, sincalide is preferable because it has been best standardized and gastric emptying is not an issue. Other uses for sincalide include the calculation of a gallbladder ejection fraction (GBEF) in patients to diagnose chronic acalculous gallbladder disease, diagnose acute acalculous cholecystitis, and differentiate biliary obstruction from functional delayed biliary clearance into the small bowel ( Box 9.3 ).
Before Tc-99m Hepatic Iminodiacetic Acid (HIDA) Examination
To empty gallbladder in patient fasting longer than 24 hours
To diagnose sphincter of Oddi dysfunction (see Box 9.15 )
After Initial 60-Minute Tc-99m HIDA Examination
Differentiate common duct obstruction from functional causes.
Exclude acute acalculous cholecystitis if gallbladder fills (rule out a false-negative study).
Diagnose chronic acalculous gallbladder disease.
The use of sincalide to empty the gallbladder in a fasting patient can result in delayed biliary-to-bowel transit. Because of its short half-life in serum, CCK can be infused a second time during a patient study (e.g., before the study in a patient who has been fasting > 24 hours and after the initial 60-minute study to calculate a GBEF). The sincalide infusion methodology should be identical for all indications, 0.02 μg/kg infused over 60 minutes.
Common Clinical Applications
Acute Cholecystitis
The most frequent indication for cholescintigraphy is to confirm or exclude the diagnosis of acute cholecystitis. Patients present with colicky right upper quadrant abdominal pain, nausea, and vomiting. Physical examination often detects right upper quadrant tenderness. Laboratory studies show leukocytosis. Liver function tests are usually normal. A confirmatory imaging study is required for the diagnosis before surgery. The cause is usually due to obstruction of the cystic duct secondary to cholelithiasis. Soon after obstruction, a series of sequential histopathological inflammatory changes occurs—first, venous and lymphatic obstruction, followed by edema of the gallbladder mucosa, then white blood cell infiltration, and, ultimately, hemorrhage, ulceration, necrosis, and if left untreated, gangrene, abscess, and perforation ( Box 9.4 ).
- 1.
Cystic duct obstruction
- 2.
Venous and lymphatic outflow obstruction
- 3.
Mucosal edema and congestion
- 4.
Neutrophilic leukocyte infiltration
- 5.
Hemorrhage and necrosis
- 6.
Gangrene, abscess
- 7.
Perforation
Imaging for Acute Cholecystitis
Ultrasonography
Most patients with acute cholecystitis have gallstones noted on sonography; however, the presence of stones is not specific for acute cholecystitis. Asymptomatic gallstones are common and may be unrelated to the cause of the abdominal pain. Other sonographic findings seen with acute cholecystitis are also nonspecific. Thickening of the gallbladder wall and peri-cholecystic fluid occur with various acute and chronic diseases. A more specific indicator of acute inflammation is intramural lucency. The sonographic Murphy sign (localized tenderness in the region of the gallbladder) is reported to have high accuracy in experienced hands; however, this finding is operator dependent and not always reliable. The combination of gallstones, intramural lucency, and the sonographic Murphy sign makes the diagnosis of acute cholecystitis likely. However, many patients with acute cholecystitis do not have all of these findings, and the diagnosis is less certain. Ultrasonography may reveal other factors causing the patient’s symptoms (e.g., common duct dilation due to biliary obstruction, pancreatic or liver tumors, renal stones, pulmonary consolidation).
Cholescintigraphy
A major advantage of HIDA scintigraphy is that it demonstrates the pathophysiology of acute cholecystitis (i.e., nonfilling of the gallbladder secondary to cystic duct obstruction). No filling by 60 minutes after Tc-99m HIDA injection is abnormal; however, it is not, by itself, diagnostic of acute cholecystitis. However, no filling on further delayed imaging at 3 to 4 hours or 30 minutes after morphine infusion is diagnostic of acute cholecystitis. Delayed filling of the gallbladder (i.e., after 60 minutes) rules out acute cholecystitis. Common reasons for delayed gallbladder filling are chronic cholecystitis and hepatic dysfunction (see Figs. 9.7–9.9 ).
Cholescintigraphy has high accuracy for the diagnosis of acute cholecystitis ( Table 9.4 ). The sensitivity (nonfilling of the gallbladder in those with the disease) is 95% to 98%, and the specificity (filling of the gallbladder in patients who do not have the disease) is > 90%. Studies that have directly compared cholescintigraphy with ultrasonography have found cholescintigraphy superior for this diagnosis (see Table 9.4 ). However, in spite of its high specificity, false-positive studies may occur. These can be minimized by anticipating the potential situations where it can happen ( Box 9.5 ) and using state-of-the-art methodology. Ensuring that patients have fasted for 3 to 4 hours before the study is critical. Those fasting > 24 hours or receiving hyperalimentation likely have a gallbladder full of viscous bile and should be administered sincalide before the study to empty the gallbladder. In these cases, false positives may still occur because of a poorly contracting gallbladder in response to CCK due to chronic cholecystitis. Patients with poor hepatic function have delayed uptake and clearance of the radiotracer and often delayed gallbladder filling. In these patients, delayed imaging for up to 24 hours may be necessary to confirm or exclude gallbladder filling; false positives may still occasionally occur.
| Sensitivity/Specificity (%) | |||
|---|---|---|---|
| Study First Author, Date | Patients | Cholescin-tigraphy | Ultrasonography |
| Stadalnik, 1978 | 120 | 100/100 | 70/93 |
| Weissmann, 1979 | 90 | 98/100 | |
| Freitas, 1980 | 186 | 97/87 | |
| Suarez, 1980 | 62 | 98/100 | |
| Szalabick, 1980 | 271 | 100/98 | |
| Weissmann, 1981 | 296 | 95/99 | |
| Zeman, 1981 | 200 | 98/82 | 67/82 |
| Worthen, 1981 | 113 | 95/100 | 67/100 |
| Mauro, 1982 | 95 | 100/94 | |
| Rails, 1982 | 59 | 86/84 | 86/90 |
| Freitas 1982 | 195 | 98/90 | 60/81 |
| Samuels, 1983 Chatziioannov, 2000 | 194 92 | 97/93 92/89 | 97/64 40/89 |
| Overall | 1988 | 97/94 | 77/84 |
Fasting <4 hours before hepatic iminodiacetic acid (HIDA) study
Fasting >24 hours before HIDA study
Parenteral alimentation
Concurrent severe illness
Chronic cholecystitis
Hepatic dysfunction
Patients with chronic cholecystitis may have false-positive findings for acute cholecystitis (nonfilling of the gallbladder) caused by a fibrotic obstruction of the cystic duct or a functional obstruction caused by a gallbladder filled with viscous bile. Even if a patient has received sincalide before the study, a diseased gallbladder, whether acute or chronic, may not contract. Very ill hospitalized patients with a concurrent serious illness may also have false-positive scintigraphic results for acute cholecystitis. The reason for this is uncertain.
False-negative results (gallbladder filling in a patient with acute cholecystitis) are rare. One important cause to be avoided is misinterpretation of the cystic duct sign, specifically cystic duct dilation proximal to its obstruction, which might be misinterpreted as a gallbladder . The focal activity is typically smaller than a gallbladder and in a more medial position ( Fig. 9.14 ).

If the gallbladder does not fill by 1 hour, either delayed imaging for up to 4 hours or morphine administration is indicated to confirm or exclude gallbladder filling. The accuracy of morphine is similar to the delayed imaging method ( Table 9.5 ) and is preferred whenever possible because it confirms or excludes the diagnosis by 30 minutes after administration. Morphine produces a functional partial common duct obstruction that cannot be differentiated by scintigraphy from a pathological partial common duct obstruction caused by stone or stricture. Thus, morphine should not be administered if scintigraphic findings show delayed clearance from the common duct and delayed transit into the small bowel. Delayed imaging is indicated for these patients. With cystic duct patency, the gallbladder begins to fill within 5 to 10 minutes after morphine infusion and is complete by 20 to 30 minutes. If no gallbladder filling is seen by the end of the 30-minute infusion, acute cholecystitis is confirmed.
| Study Author, Date | Patients | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| Choy, 1984 | 59 | 96 | 100 |
| Keslar, 1987 | 31 | 100 | 83 |
| Vasquez, 1987 | 40 | 100 | 85 |
| Fig, 1990 | 51 | 94 | 69 a |
| Flancbaum, 1994 | 75 | 99 | 91 |
| Fink-Bennett, 1991 | 51 | 95 | 99 |
| Kistler, 1991 | 32 | 93 | 78 a |
| Overall | 339 | 96 | 86 |
a High percentage of patients with concurrent illness and chronic cholecystitis.
Ancillary Scintigraphic Findings of Acute Cholecystitis
Increased blood flow to the gallbladder fossa secondary to severe inflammation is seen in some patients (see Fig. 9.9 ). Increased hepatic uptake of HIDA tracer adjacent to the gallbladder fossa in patients with acute cholecystitis is called the rim sign ( Fig. 9.15 ) and is seen in approximately 25% of patients with acute cholecystitis. The rim sign is more common than increased flow to the gallbladder fossa. Sometimes they occur together. The rim sign can usually be seen throughout the duration of the study but is best seen as the radiotracer clears from the uninvolved liver. It is caused by inflammation of the liver adjacent to the gallbladder fossa. With severe acute cholecystitis, inflammation may spread to the adjacent normal liver, which can result in increased blood flow to that region, increased radiotracer delivery, and thus increased Tc-99m HIDA hepatic extraction.

The importance of the rim sign is twofold. First, it is a very specific scintigraphic finding of acute cholecystitis. It increases interpretive confidence that nonfilling of the gallbladder is caused by acute cholecystitis (true positive) in a patient at increased risk for a false-positive study (see Box 9.5 ), for example, a sick hospitalized patient with concurrent serious illness. Second, the rim sign identifies patients with acute cholecystitis who have more severe disease and are at increased risk for complications (e.g., gangrene and perforation). Even without these complications, patients with the rim sign tend to be sicker and at a later stage of the pathophysiological spectrum of disease, with hemorrhage and necrosis rather than edema and leukocyte infiltration (see Box 9.4 ).
Acute Acalculous Cholecystitis
The acalculous form of acute cholecystitis is not common; however, it can be life-threatening. It occurs in seriously ill hospitalized patients, often those in the intensive care unit (ICU; Box 9.6 ). Because of its high mortality (30%) and morbidity (55%), early diagnosis is imperative; however, because of concomitant serious illness, diagnosis is often delayed. In the majority of patients, acute acalculous cholecystitis is initiated by cystic duct obstruction but not by cholelithiasis, rather, by inflammatory debris, inspissated bile, and local edema, aggravated by dehydration. To complicate the diagnosis further, some of these patients do not have cystic duct obstruction but, rather, direct inflammation of the gallbladder wall caused by systemic infection, ischemia, or toxemia. This results in a lower diagnostic sensitivity for HIDA imaging.
Postoperative
Multiple trauma
Extensive burns
Shock
Acquired immunodeficiency syndrome
Mechanical ventilation
Multiple transfusions
Vasculitis
The sensitivity of cholescintigraphy for diagnosis of acute acalculous cholescintigraphy is approximately 80%, compared with 95% to 98% for acute calculous cholecystitis ( Table 9.6 ). The lower sensitivity is at least partially due to the fact that some of these patients do not have cystic duct obstruction. If a false-negative study result (filling of the gallbladder in acute acalculous cholecystitis) is suspected in a patient with a high clinical suspicion, sincalide infusion with a gallbladder ejection fraction can be helpful. An acutely inflamed gallbladder does not contract normally. Good contraction excludes the diagnosis of cholecystitis. Poor contraction is consistent with cholecystitis but not necessarily acute cholecystitis. It could be caused by chronic cholecystitis, medications that inhibit contraction, or concomitant acute or chronic illness ( Boxes 9.7 and 9.8 ). In uncertain cases, a radiolabeled leukocyte study could confirm the diagnosis. Although it is urgent for these sick patients to have gallbladder surgery, the increased risk of surgery may call for more certainty and a willingness to wait for the leukocyte study. Indium-111 (In-111) leukocytes are preferable because they have no intraabdominal clearance. Tc-99m-labeled leukocytes are cleared through the biliary and urinary system. However, early-same-day Tc-99m HMPAO leukocyte imaging at 1 to 2 hours, before biliary clearance occurs, may avoid this problem. Although the standard imaging time for In-111 leukocytes is at 24 hours, imaging at 4 hours may be diagnostic if gallbladder uptake is seen.
| Study Author, Date | Patients | Sensitivity (%) | Specificity (%) |
|---|---|---|---|
| Shuman, 1984 | 19 | 68 | |
| Weissmann, 1983 | 15 | 93 | |
| Mirvis, 1986 | 19 | 90 | 61 |
| Swayne, 1986 | 49 | 93 | |
| Ramanna, 1984 | 11 | 100 | |
| Flancbaum, 1995 | 16 | 75 | 100 |
| Prevot, 1999 | 14 | 64 | 100 |
| Mariat, 2000 | 12 | 67 | 100 |
| Overall | 155 | 81 | 90 |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


