KEY FACTS
Terminology
- •
Hepatocellular carcinoma (HCC)
- ○
Primary malignancy of liver arising from hepatocytes
- ○
- •
Synonyms: Hepatoma, primary liver cancer
Imaging
- •
Ultrasound: Primary test for screening/surveillance for HCC
- ○
Solid, intrahepatic mass may be hypoechoic (most common), hyperechoic, or isoechoic
- ○
May see hypoechoic halo, mild posterior acoustic enhancement, or internal vascularity on color Doppler
- ○
Infiltrative tumors often difficult to visualize margins; look for refractive edge shadows, parenchymal distortion, or loss of normal echogenic portal triads, which are helpful secondary findings
- ○
Portal vein or hepatic vein tumor invasion highly suggestive of HCC
- ○
- •
Contrast-enhanced CT, MR, or CEUS: For characterization
- ○
Arterial hyperenhancement and portal/delayed washout
- ○
Top Differential Diagnoses
- •
Intrahepatic cholangiocarcinoma
- •
Regenerative or dysplastic nodule
- •
Hepatic hemangioma (especially hyalinized subtype)
- •
Focal nodular hyperplasia
- •
Hepatic adenoma
- •
Metastases
Clinical Issues
- •
Screening/surveillance ultrasound every 6 months recommended for the following populations in USA
- ○
Cirrhosis (60-90%) from any cause
- –
Most commonly due to chronic viral hepatitis (HBV, HCV), alcoholic cirrhosis
- –
- ○
Noncirrhotic chronic Hepatitis B in certain populations
- –
Asian male > 40, Asian female > 50, African/North American black, family history HCC
- –
- ○
Surveillance benefit uncertain in following populations: Noncirrhotic chronic HCV with stage 3 fibrosis, noncirrhotic nonalcoholic fatty liver disease, and noncirrhotic HBV carriers with active hepatitis who do not meet above criteria
- ○
Scanning Tips
- •
Careful inspection of portal veins and hepatic veins for thrombus critical; infiltrative HCC often invades veins
- •
Liver dome lesions are often missed; angle transducer to image above HV to completely visualize liver dome
- •
RT and LT inferior tip of liver lesions are easily missed; carefully scan through very inferior portions of liver
- •
Anterior lesions often poorly visualized with curvilinear or vector transducers; diligent use of 9-MHz linear probe helps visualization of superficial portions of liver
- •
Trying multiple probes, positions, and windows are key to improve detection; some liver lesions may only be seen on left lateral decubitus position (vs. supine) or intercostal approach (vs. subcostal)
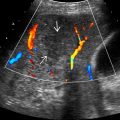
 . Numerous adjacent satellite nodules
. Numerous adjacent satellite nodules  and portal vein invasion
and portal vein invasion  are depicted. Underlying liver disease is evident given the nodular liver capsule
are depicted. Underlying liver disease is evident given the nodular liver capsule  and ascites
and ascites  .
.Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


