Manifestations of atherosclerotic plaque in different arterial beds range from perfusion deficits to overt ischemia such as stroke and myocardial infarction. Atherosclerotic plaque composition is associated with its propensity to rupture and cause vascular events. Magnetic resonance (MR) imaging of atherosclerotic plaque using clinical 1.5 T scanners can detect plaque composition. Plaque MR imaging at higher field strengths offers both opportunities and challenges to improving the high spatial resolution and contrast required for this type of imaging. This article summarizes the technological requirements required for high-field plaque MR imaging and its application in detecting plaque components.
- •
Increased SNR (signal-to-noise ratio) at 3 T has allowed new three-dimensional (3D) isotropic sequences with large coverage to be developed with improved slice resolution compared with 1.5 T.
- •
Criteria for identification of plaque components at 1.5 T are also applicable at 3 T with minor differences for intraplaque hemorrhage (IPH) and calcification.
- •
Signal from IPH is reduced on time of flight (TOF) compared with 1.5 T because of longer T1 relaxation times at 3 T. Dedicated sequences such as magnetization prepared rapid gradient echo (MPRAGE) can improve both sensitivity and specificity for hemorrhage detection.
- •
Calcifications are larger at 3 T because of increased susceptibility effects.
- •
High-field plaque imaging is possible in multiple arterial beds such as carotids, peripheral arteries, and aorta. Intracranial vessel wall imaging is also improved at 3 T. Challenges such as motion, field inhomogeneities, susceptibility, and specific absorption rate (SAR) are yet to be overcome for routine coronary plaque magnetic resonance (MR) imaging.
The following morphologic features represent important information that can be obtained though high-field atherosclerotic plaque imaging:
Atherosclerotic plaque size
- •
Intraplaque hemorrhage (IPH)
- •
Lipid-rich necrotic core (LRNC) size
- •
Luminal stenosis/ulcer
- •
Calcification
- •
High-field plaque MR imaging
Plaque MR imaging requires a high SNR for acquisition for several reasons: (1) because of the small size of its imaging target, atherosclerotic plaque MR imaging needs to be acquired at high spatial resolution to faithfully characterize the morphology of the plaque; (2) to visualize the plaque on vessel wall, the bright luminal signal needs to be suppressed; (3) to accomplish large coverage scans in a clinical feasible time also demands a higher SNR to avoid compromised image quality.
Three areas of technological improvements can improve the SNR and contrast between vessel wall, lumen, and the outer wall: scanner field strength, surface radiofrequency (RF) coils and vessel wall imaging sequences. Each of these areas is addressed later along with their respective challenges arising from high-field imaging. Following this, advances in knowledge of the atherosclerotic disease process using these new technologies are described. Throughout this article, 3 T is considered as high-field; 7 T and greater are considered ultrahigh-field.
High-field MR scanners
Compared with lower field strengths, higher field strength promises higher overall SNR. Theoretic analysis predicts that the SNR of the MR imaging system will increase by 100% if the main magnetic field is doubled (eg, from 1.5 T to 3 T). This increased SNR is the primary motivation for moving plaque MR imaging to high-fields. Although the SNR improvement in vivo can vary for different applications, this overall improvement makes high-field MR imaging a preferable platform for plaque imaging compared with 1.5 T. The SNR gain can be traded for shortened imaging time, higher spatial resolution, or a combination of the two depending on the imaging needs. Nevertheless, increased magnetic field strengths also represent new challenges, such as prolonged T1 relaxation time, increased field inhomogeneity, and susceptibility.
Whole-body MR scanners at 1.5 T and 3 T are now well established for vessel wall imaging. 3 T provides an improved contrast/noise ratio of 1.4 to 2.4 times compared with 1.5 T black blood (BB) MR imaging. Wide-bore magnets are also desirable, because large patients are generally prone to atherosclerosis.
Fat suppression is necessary in vessel wall imaging to delineate the outer wall. Thus, field inhomogeneity can be challenging at higher field strengths for achieving good fat suppression. Good first-order shimming routines are often adequate for vessel wall imaging. In a few cases, higher order shimming may be necessary. Newer MR systems are equipped with RF shimming capabilities and may prove useful for vessel wall MR imaging.
RF Coils
Body coil transmission is used for vessel wall imaging and is useful for uniform excitation and the large coverage needed for special blood suppression techniques. However, body coil reception does not provide high enough SNR for visualizing the vessel wall. Surface coils pick up signal from a small area, but with increased sensitivity. Because the carotid arteries are superficial, they can be imaged with surface coils to increase SNR. Surface coils with 4, 6, and 8 coil elements have been developed for use at 3 T. Dedicated 4-element phased array coils enable high-resolution imaging at 1.5 T and 3 T. Increasing the number of coil elements provides larger coverage. An 8-element carotid coil not only provided a 1.7-fold SNR increase compared with a 4-element design but also provided increased coverage along the length of the carotid artery. Currently, carotid phased array coils with 4, 6, and 8 coil elements are available commercially on the major scanner platforms. Fig. 1 shows the design of the 8-element coil and its commercial equivalent. Each coil element is usually read out through a separate RF channel. The noise picked up by the receive chain can be further reduced by digitizing the signal from the coil elements. Newer MR systems digitize the received signal directly at the coil, thereby reducing noise picked up in each of the channels. Such systems can further improve the performance of these coils but require additional components on the coil to digitize the received signal. Improvements in both coil design and the RF receive chain allow plaque imaging with higher SNR and therefore enable higher spatial resolution to be attained. Such improvements will benefit vessel wall imaging in vascular beds such as coronary and intracranial vasculature where high spatial resolution (<0.5 mm in plane) is required.
3D BB Imaging Sequences
Compared with its two-dimensional (2D) counterparts, 3D imaging sequences present several advantages for atherosclerotic plaque imaging. Benefiting from the extra phase encoding direction, a 3D imaging sequence provides significant SNR enhancement because the imaging volume expands in the third dimension. This extra SNR advantage can be used to achieve isotropic resolution, because previous studies have shown that isotropic voxels can potentially reduce registration and segmentation errors, as well as provide more reproducible quantitative measurements for vessel wall imaging.
Despite these benefits, achieving high-resolution 3D isotropic resolution in vivo is challenging. Depending on the field strength, achieving isotropic resolutions may require long scan times. As a result, many of the 3D implementations on 1.5 T have adopted anisotropic voxel size to accommodate clinical needs.
The improved SNR offered by high magnetic field strength provides a potential solution to this issue. Recently a 3D turbo spin echo (TSE) with variable flip angle refocusing RF pulses (SPACE) technique was used to achieve high-resolution isotropic (0.72 × 0.72 × 0.72 mm 3 ) large coverage (380 × 374 × 100 mm 3 ) peripheral artery imaging at 3 T. The whole volume can be acquired in 11.32 minutes. A similarly configured 2D sequence would need 20 minutes to cover the same volume at a lower slice direction resolution of 3 mm.
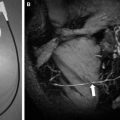
Motion-sensitized driven equilibrium (MSDE) is a new imaging technique that can effectively suppress blood signal by dephasing moving spins in the blood. When combined with proper acquisition schemes, high temporal efficiency can be achieved. In only 2 minutes, the carotid artery tree can be imaged using a 3D MSDE prepared rapid gradient echo (3D-MERGE) sequence with high spatial resolution (0.7 × 0.7 × 0.7 mm 3 ) and large coverage (250 mm foot to head direction) ( Fig. 2 ). More importantly, recent research reveals that the 3D-MERGE sequence is not restricted to plaque burden measurement, but can also be used to detect high-risk plaque components if the parameters are properly optimized. Two separate studies have shown the usefulness of 3D-MERGE to detecting LRNC and IPH. These findings suggest that the optimization toward plaque imaging with higher temporal efficiency does not rule out its potential for simultaneous high-risk plaque component detection.
High-field plaque MR imaging
Plaque MR imaging requires a high SNR for acquisition for several reasons: (1) because of the small size of its imaging target, atherosclerotic plaque MR imaging needs to be acquired at high spatial resolution to faithfully characterize the morphology of the plaque; (2) to visualize the plaque on vessel wall, the bright luminal signal needs to be suppressed; (3) to accomplish large coverage scans in a clinical feasible time also demands a higher SNR to avoid compromised image quality.
Three areas of technological improvements can improve the SNR and contrast between vessel wall, lumen, and the outer wall: scanner field strength, surface radiofrequency (RF) coils and vessel wall imaging sequences. Each of these areas is addressed later along with their respective challenges arising from high-field imaging. Following this, advances in knowledge of the atherosclerotic disease process using these new technologies are described. Throughout this article, 3 T is considered as high-field; 7 T and greater are considered ultrahigh-field.
High-field MR scanners
Compared with lower field strengths, higher field strength promises higher overall SNR. Theoretic analysis predicts that the SNR of the MR imaging system will increase by 100% if the main magnetic field is doubled (eg, from 1.5 T to 3 T). This increased SNR is the primary motivation for moving plaque MR imaging to high-fields. Although the SNR improvement in vivo can vary for different applications, this overall improvement makes high-field MR imaging a preferable platform for plaque imaging compared with 1.5 T. The SNR gain can be traded for shortened imaging time, higher spatial resolution, or a combination of the two depending on the imaging needs. Nevertheless, increased magnetic field strengths also represent new challenges, such as prolonged T1 relaxation time, increased field inhomogeneity, and susceptibility.
Whole-body MR scanners at 1.5 T and 3 T are now well established for vessel wall imaging. 3 T provides an improved contrast/noise ratio of 1.4 to 2.4 times compared with 1.5 T black blood (BB) MR imaging. Wide-bore magnets are also desirable, because large patients are generally prone to atherosclerosis.
Fat suppression is necessary in vessel wall imaging to delineate the outer wall. Thus, field inhomogeneity can be challenging at higher field strengths for achieving good fat suppression. Good first-order shimming routines are often adequate for vessel wall imaging. In a few cases, higher order shimming may be necessary. Newer MR systems are equipped with RF shimming capabilities and may prove useful for vessel wall MR imaging.
RF Coils
Body coil transmission is used for vessel wall imaging and is useful for uniform excitation and the large coverage needed for special blood suppression techniques. However, body coil reception does not provide high enough SNR for visualizing the vessel wall. Surface coils pick up signal from a small area, but with increased sensitivity. Because the carotid arteries are superficial, they can be imaged with surface coils to increase SNR. Surface coils with 4, 6, and 8 coil elements have been developed for use at 3 T. Dedicated 4-element phased array coils enable high-resolution imaging at 1.5 T and 3 T. Increasing the number of coil elements provides larger coverage. An 8-element carotid coil not only provided a 1.7-fold SNR increase compared with a 4-element design but also provided increased coverage along the length of the carotid artery. Currently, carotid phased array coils with 4, 6, and 8 coil elements are available commercially on the major scanner platforms. Fig. 1 shows the design of the 8-element coil and its commercial equivalent. Each coil element is usually read out through a separate RF channel. The noise picked up by the receive chain can be further reduced by digitizing the signal from the coil elements. Newer MR systems digitize the received signal directly at the coil, thereby reducing noise picked up in each of the channels. Such systems can further improve the performance of these coils but require additional components on the coil to digitize the received signal. Improvements in both coil design and the RF receive chain allow plaque imaging with higher SNR and therefore enable higher spatial resolution to be attained. Such improvements will benefit vessel wall imaging in vascular beds such as coronary and intracranial vasculature where high spatial resolution (<0.5 mm in plane) is required.
3D BB Imaging Sequences
Compared with its two-dimensional (2D) counterparts, 3D imaging sequences present several advantages for atherosclerotic plaque imaging. Benefiting from the extra phase encoding direction, a 3D imaging sequence provides significant SNR enhancement because the imaging volume expands in the third dimension. This extra SNR advantage can be used to achieve isotropic resolution, because previous studies have shown that isotropic voxels can potentially reduce registration and segmentation errors, as well as provide more reproducible quantitative measurements for vessel wall imaging.
Despite these benefits, achieving high-resolution 3D isotropic resolution in vivo is challenging. Depending on the field strength, achieving isotropic resolutions may require long scan times. As a result, many of the 3D implementations on 1.5 T have adopted anisotropic voxel size to accommodate clinical needs.
The improved SNR offered by high magnetic field strength provides a potential solution to this issue. Recently a 3D turbo spin echo (TSE) with variable flip angle refocusing RF pulses (SPACE) technique was used to achieve high-resolution isotropic (0.72 × 0.72 × 0.72 mm 3 ) large coverage (380 × 374 × 100 mm 3 ) peripheral artery imaging at 3 T. The whole volume can be acquired in 11.32 minutes. A similarly configured 2D sequence would need 20 minutes to cover the same volume at a lower slice direction resolution of 3 mm.
Motion-sensitized driven equilibrium (MSDE) is a new imaging technique that can effectively suppress blood signal by dephasing moving spins in the blood. When combined with proper acquisition schemes, high temporal efficiency can be achieved. In only 2 minutes, the carotid artery tree can be imaged using a 3D MSDE prepared rapid gradient echo (3D-MERGE) sequence with high spatial resolution (0.7 × 0.7 × 0.7 mm 3 ) and large coverage (250 mm foot to head direction) ( Fig. 2 ). More importantly, recent research reveals that the 3D-MERGE sequence is not restricted to plaque burden measurement, but can also be used to detect high-risk plaque components if the parameters are properly optimized. Two separate studies have shown the usefulness of 3D-MERGE to detecting LRNC and IPH. These findings suggest that the optimization toward plaque imaging with higher temporal efficiency does not rule out its potential for simultaneous high-risk plaque component detection.
Challenges and opportunities of high-field plaque MR imaging
Increased Field Inhomogeneity
The magnetic field inhomogeneity describes the level of field fluctuation in the image field of view. Two types of field inhomogeneities are present: the inhomogeneity of the main magnetic field (B0 inhomogeneity), and the inhomogeneity of the transmission RF field (B1 inhomogeneity). In high-field MR systems, both fields are more susceptible to variations than at lower field strengths, especially for complicated anatomic regions like the neck, which is a common target of plaque imaging. It is therefore more important to design new sequences to compensate for these inhomogeneities.
The MSDE BB imaging technique can provide robust blood suppression even in challenging anatomic regions. It relies on dephasing among moving particles to achieve BB effect. Because it does not put any direct requirement on flow velocity like other BB techniques do, MSDE can suppress blood more effectively in regions of complex blood flow.
A practical problem with MSDE at high-field is its sensitivity to B1 inhomogeneity. As shown in Fig. 3 , when the B1 value drifts away from the nominal value (ie, relative B1 drifts away from 1), significant signal reduction can be observed on the MSDE sequence. At high-fields, SNR can vary across the field of view because of this B1 sensitivity.
To address this issue, an improved MSDE (iMSDE) sequence was proposed. In the iMSDE sequence, the original 90-180-90 RF chain was replaced by the MLEV-4 pulse train ( Fig. 4 ), which is known to be more robust to B1 inhomogeneity. Almost no noticeable signal decrease could be observed on the iMSDE pulses in Fig. 3 even when significant inhomogeneity is present (toward the periphery of the image).
Related posts:
 Stroke: High-Field Magnetic Resonance Imaging
Current State-of-the-Art 1.5 T and 3 T Extracranial Carotid Contrast-Enhanced Magnetic Resonance Angiography
Stroke: High-Field Magnetic Resonance Imaging
Current State-of-the-Art 1.5 T and 3 T Extracranial Carotid Contrast-Enhanced Magnetic Resonance Angiography
 Vascular Disorders: Insights from Arterial Spin Labeling
Vascular Disorders: Insights from Arterial Spin Labeling
 Current Status and Future Perspectives of Magnetic Resonance High-Field Imaging: A Summary
Current Status and Future Perspectives of Magnetic Resonance High-Field Imaging: A Summary
 Pediatric High-Field Magnetic Resonance Imaging
Pediatric High-Field Magnetic Resonance Imaging
 Ultrahigh-Field Magnetic Resonance Imaging: The Clinical Potential for Anatomy, Pathogenesis, Diagnosis and Treatment Planning in Neck and Spine Disease
Ultrahigh-Field Magnetic Resonance Imaging: The Clinical Potential for Anatomy, Pathogenesis, Diagnosis and Treatment Planning in Neck and Spine Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


