Fig. 18.1
Pneumonia complicating human infection of avian influenza (H5N1). (a) At day 5 after the onset, X-ray demonstrates small flakes of light blurry shadow at the left upper lung. (b) At day 9 after the onset, the lesions at the left upper lung rapidly spread to the upper and middle lung fields with accompanying pulmonary tissue atrophy and collapse and inner air bronchus sign. The right lung is demonstrated with patches of blurry shadow at the medial part. (c) At day 13 after the onset, the lesions at the left lung spread to the whole lung with white lung sign. The pulmonary atrophy and collapse are aggravated. And the right lung is demonstrated with more lesions. (d) At day 15 after the onset, CT scanning demonstrates collapse of the left thorax, large quantities of flakes, and cord-like shadow at the left lung and the upper right lung lobe with inner air bronchus sign. Some pulmonary tissues herniate into the anterior-posterior mediastinum with leftward shift of the mediastinum. (e) At day 22 after the onset, HRCT demonstrates that all lesions at both lungs are absorbed but aggravated atrophy and collapse of the left lung tissue as well as aggravated mediastinal herniation. (f) At day 31 after the onset, the lesions at both lungs are obviously absorbed. The absorption at the left anterolateral lung is more obvious than that at the posteromedial lung. (g) At day 53 after the onset, HRCT demonstrates more cord-like shadow at the left upper lung with grid-like change. The right upper lung lobe is demonstrated with small quantities of cord-like shadow and ground-glass opacity, with leftward shift of the mediastinum. (h) By reexamination after 11 months, CT scanning still demonstrates cord-like shadow and slight leftward shift of the mediastinum
Fig. 18.2
Pneumonia complicating human infection of avian influenza (H5N1). (a) At day 6 after the onset, X-ray demonstrates large flakes of high-density shadow at the left upper lung, patches of blurry shadow at the right upper lung, and slightly narrowed left intercostal space. (b) At day 7 after the onset, the lesions at both lung increase obviously. (c) By reexamination after 8 months, CT scanning demonstrates that some ground-glass opacity and inferior line of the pleura at the left upper lung
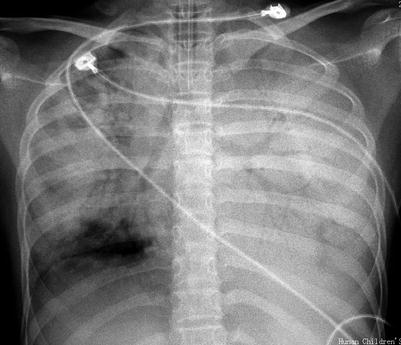
Fig. 18.3
Pneumonia complicating human infection of avian influenza H5N1. At day 4 after the onset, X-ray demonstrates diffuse consolidation at both lungs with inner air bronchus sign
Fig. 18.4
Pneumonia complicating human infection of avian influenza (H5N1). (a) At day 6 after the onset, the left middle and lower lung fields are demonstrated with large flakes of shadows with increased density and poorly defined boundary. Some lesions are demonstrated as ground-glass opacity and the left hilum is poorly defined. (b) At day 8 after the onset, the conditions progress rapidly with large flakes of increased density shadow at the left lung in white lung sign. Flakes of increased density shadow are demonstrated at the right hilar area, right middle lung, as well as middle and medial parts of the right lower lung field. (c) At day 9 after the onset, the left lung field is demonstrated with large flakes of shadow and the right lung is demonstrated with slightly larger range with lesions. (d) At day 10 after the onset, the left lower lung field is demonstrated with slightly light shadow indicating partially absorption of some lesions. The right lung is demonstrated with obviously larger range with lesions. (e) At day 11 after the onset, the left upper and middle lung fields are demonstrated with slightly light shadows. The right lung is demonstrated with continued expansion of the range with lesions of increased density, especially at the right middle and lower lung fields. (f) At day 14 after the onset, the shadows at the left middle and lower lung fields as well as at the middle and lateral parts of right middle and lower lung fields are demonstrated to be lightened, indicating absorption of some lesions. (g) At day 20 after the onset, both lungs are demonstrated with patches of shadows. The middle and lateral parts of both middle lung fields are demonstrated with small flakes of light blurry shadows. The left lower lung field is demonstrated with slight decreased transparency. The left costophrenic angle is demonstrated to be poorly defined. (h) At day 22 after the onset, the right lung field is demonstrated with patches and large flakes of consolidation shadows. The left lung field is demonstrated with diffuse increased density shadows. The left diaphragmatic surface and left costophrenic angle are poorly defined. The conditions progressed. (i) At day 28 after the onset, the left lung is demonstrated with diffuse increased density consolidation. The right lung is demonstrated with large flakes and patches of shadows. Some lung fields are demonstrated with increased transparency. The mediastinum is demonstrated with slight shift leftwards. (j) At day 30 after the onset, the left lung is demonstrated with systemic increased density consolidation shadow. The right lung is demonstrated with large flakes and patches of shadows, with slightly more lesions. (k) At day 32 after the onset, the right middle and lower lung is demonstrated with large flakes and cord-like shadows. The left middle and lower lung is demonstrated with systemic increased density consolidation shadow. The lesions at the right lung and the left upper lung are absorbed, with improved transparency. (l) At day 34 after the onset, the right lung is demonstrated with patches and cord-like increased density shadows. The left lung is demonstrated with systemic light increased density shadows. The lesions at both lungs are obviously absorbed. (m) At day 47 after the onset, the medial part the right lower lung is demonstrated with dense strips of shadows, with poorly defined right heart margin. The left lung is demonstrated with dense cord-like shadows, with well-defined boundary, patches, and spots of shadows as well as less cord-like shadows. (n) At day 53 after the onset, both middle and lower lung fields are demonstrated with less patches of high-density shadows, with scattering cord-like shadows and well-defined boundary. The lesion at the right cardiophrenic angle is demonstrated with cystic dilation of bronchus. Most fields of both lungs are demonstrated with no abnormality. (o) At day 79 after the onset, both lungs are demonstrated with scattering patches and cord-like high-density shadows that are well defined. The lesions are characterized by fibrosis. (p) At day 172 after the onset, both lungs are demonstrated with scattering spots and cord-like high-density shadows with well-defined boundary
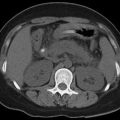
Fig. 18.5
Pneumonia complicating human infection of avian influenza (H5N1). (a–h) At day 7 after the onset, CT scanning demonstrates light small flakes of shadows at the posterior segment of the right upper lung lobe and medial segment of the right middle lung lobe. The apical posterior and anterior segments of the left upper lung lobe are demonstrated with irregular small flakes of consolidation shadows. The lingual segment of the upper lung lobe and most segments of the lower lung lobe are demonstrated with large flakes of dense consolidation shadow, with inner air bronchus sign. The left pleural cavity is demonstrated with rare liquid density shadow. (i) The liver and spleen are subject to obvious enlargement and diffuse lesion. (j–o) At day 172 after the onset, CT scanning demonstrates that the lesions at both lungs are fibrous cord-like and grid-like shadows, rigidity of some vascular markings, and no obvious absorption of the lesions. (p–s) At day 286 after the onset, CT scanning demonstrates that the lesions at both lungs are still mainly changes of pulmonary interstitial tissues, such as fibrous cord-like and grid-like shadows, with slow absorption of the lesions. (t–y) At day 730 after the onset, reexamination by CT scanning demonstrates that the lesions at both lungs are still mainly changes of pulmonary interstitial tissues, such as fibrous cord-like and grid-like shadows with rare ground-glass opacity. Compare to previous chest CT findings; the lesions at both lungs are slightly absorbed
18.7.2 Dynamic Change of Thoracic Lesion
Chest X-ray demonstrations of human infected avian influenza are characterized by their rapid change, which is also an important difference from common pneumonia and other atypical pneumonia. At the early and progressive stages, the lung lesions are subject to rapid changes during a short period of time (the shortest period being 12 h), with expansion, perfusion, and migration of the lesions. The shape, range, and location of the lesions may also be subject to changes.
The absorption of lesions generally occurs 14 days after the onset, but in rare mild type of cases, it may occur at day 7 after the onset, with decreased range and density of lesions. For those with favorable therapeutic effect, the large flakes of shadow at the lungs can be significantly changed within 1 day. ARDS is the main cause of death in patients with avian influenza. In severe cases, diffuse alveolar consolidation and ground-glass opacity can be demonstrated at the lungs. Preliminary observations demonstrate that in the cases of death extensive pulmonary consolidation and white lung sign are commonly demonstrated during the progressive stage.
18.7.3 Characteristic Radiological Demonstrations of Chest
1.
At the early stage after the onset, large flakes of shadow with increased density and ground-glass opacity can be demonstrated at the lungs.
2.
The invasion to lung tissues by avian influenza virus is extensive, characterized by multilobar, multi-segmental, diffuse exudative lesions at both lungs. At the peak of their development, white lung sign can be demonstrated.
3.
Rapid development of the lesions is demonstrated by radiological examination.
4.
Both pulmonary parenchyma and interstitium are simultaneously involved. Therefore, chest radiology is characterized by alveolar exudation and pulmonary consolidation.
5.
Slow absorption of the lesions is demonstrated.
Case Study 1
A boy aged 6 years complained of fever and cough for 15 days, which aggravated with accompanying chest distress, shortness of breath, headache, and muscle soreness for 1 week. He lived in a region with deaths of diseased chicken and ducks and he had a history of intake of diseased chicken and duck. Real-time PCR of pharyngeal swab and RT-PCR demonstrated positive nucleic acids of avian influenza virus H5N1. His mother died from respiratory failure on the day when the boy experienced the onset 7 days after her complaint of high fever and cough.
Case Study 2
A boy aged 9 years complained of cough for 8 days and fever for 4 days. He lived in a region with recent deaths of diseased duck and he had a history of intake of dead duck. By laboratory test, his pharyngeal swab and serum test demonstrated negative H5N1 virus. And paired serum at the advanced and convalescent stages demonstrated above 4 times increase of the specific antibody against H5N1.
Case Study 3
A girl aged 12 years who was the elder sister of the boy in Case Study 2 complained of fever for 5 days, cough and cyanosis at the lips for 2 days, as well as dyspnea for half a day. She lived in a region with recent deaths of diseased duck and she had a history of intake of dead duck. By laboratory test, serum test demonstrated negative H5N1 virus. At day 5 after the onset, her conditions aggravated and death occurred due to multiple organ failure.
Case Study 4
A male patient aged 47 years who was a driver experienced onset on June 6, 2006, and was hospitalized due to fever and cough. He denied a definite epidemiological history. Laboratory test demonstrated positive H5N1 virus.
18.7.4 Imaging Demonstrations of Human Infected Avian Influenza (H7N9)
The cases complicated by pneumonia are radiologically demonstrated with flakes of shadow at the lungs. In severe cases, the conditions progress rapidly, with ground-glass opacity, pulmonary consolidation shadow, and accompanying small quantity of pleural effusion (Figs. 18.6, 18.7, 18.8, and 18.9). In the cases with ARDS, the lesions are extensively distributed.
Fig. 18.6
Pneumonia complicating human infection of avian influenza (H7N9). (a) At day 4 after the onset, X-ray demonstrates small flakes of dense shadow at the left lower lung field and small flakes of light blurry shadows at the right lower lung field. The left costophrenic angle is poorly defined and the pulmonary markings at the right lung are also enhanced. (b) At day 5 after the onset, X-ray demonstrates large flakes of dense shadow at the left middle and lower lung fields as well as scattering patches of shadows at the right lung. The conditions progress. (c) At day 6 after the onset, the range with lesions at the right lung is enlarged. (d) At day 7 after the onset, X-ray demonstrates strips of dense shadow at the right middle lung field with inner cavity-like lesion. The conditions progress. (e) At day 8 after the onset, the lesions show no obvious change. (f) At day 12 after the onset, the lesions are obviously absorbed, but dense shadows are demonstrated at the lateral part of the left lower lung field. (g) At day 14 after the onset, the lesions at the left lower lung field are absorbed obviously. (h) At day 18 after the onset, the lesions at both lungs are completely absorbed, with clearly defined lung markings and no enlarged hilar shadow (Note: The case and the figures were provided by Zhao QX and Yang YJ from Infectious Diseases Hospital, Zhengzhou, Henan, China)
Fig. 18.7




Pneumonia complicating human infection of avian influenza (H7N9). (a) At day 4 after the onset, X-ray demonstrates large flakes of high-density shadows at the left lower lung field and overlapping of some lesions with the heart shadow. (b) At day 5 after the onset, X-ray demonstrates large flakes of ground-glass opacity and consolidation shadows at the left lung. The left costophrenic angle and diaphragmatic surface are poorly defined. The right upper lung field is demonstrated with large flakes of increased density shadows with thickened horizontal fissure. Compared to the previous X-ray finding, the range with lesions at both lungs is obviously enlarged. (c–f) At day 6 after the onset, CT scanning demonstrates flakes of ground-glass opacity at the right upper lung and left lower lung, with consolidation shadow at the left lower lung and a little pleural effusion at the right side. (g–i) At day 12 after the onset, reexamination by CT scanning demonstrates that the lesions at the right lung are basically absorbed while most of the lesions at the left lower lung are absorbed, but still with patches of shadows. The clinical symptoms are obviously alleviated. (j, k) At day 18 after the onset, CT scanning demonstrates slight absorption of the lesions at the left lung and left pleural effusion. (l, m) At day 25 after the onset, chest CT scanning demonstrates the lesions at the left lung continue to be absorbed and left pleural effusion is absorbed apparently
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
