Anatomy, embryology, pathophysiology
- ◼
Extraluminal air is a worrisome finding that should immediately heighten the suspicion of the radiologist to a potentially life-threatening complication.
- ◼
The gastrointestinal (GI) tract is lined by inner circular and outer longitudinal muscularis layers, except for the stomach, which contains a trilaminar muscularis externa.
- ◼
True diverticula (e.g., Meckel diverticulum) contain all three layers of intestinal wall, whereas false diverticula (such as within the sigmoid colon) represent focal outpouchings of mucosa, submucosa, or muscularis mucosa through defects within the wall.
- ◼
Once a lumen becomes obstructed, continual mucus secretion and bacterial overgrowth lead to increased intraluminal pressure, vascular compromise, and perforation.
- ◼
Air has a tendency to collect within the space where injury has occurred, whether that is intraperitoneal in cases of small bowel perforation, retroperitoneal if involving the duodenum/descending colon, or in the mediastinum when affecting the esophagus.
- ◼
Free air is 95% specific, but only 30% to 60% sensitive for bowel injury.
- ◼
Extravasation of oral contrast has a relatively low sensitivity (19%–42%), because of resealing of smaller perforations.
- ◼
Symptoms may be initially localized to the source of disease; however, once perforation progresses to generalized peritonitis, symptoms usually include shock, guarding, and prostration.
Techniques
Radiography
- ◼
May be used as an initial screening tool in cases of suspected perforation; however, sensitivity for detecting small volume pneumoperitoneum is limited.
- ◼
In addition to supine imaging, erect and left lateral decubitus views help increase sensitivity ( Figs. 4.1 and 4.2 ).

Fig. 4.1
Erect single view radiograph of the abdomen demonstrates free air under the diaphragm ( asterisk ). Air may also be seen on both sides of a loop of bowel in the left upper quadrant (Rigler’s sign) ( arrows ).
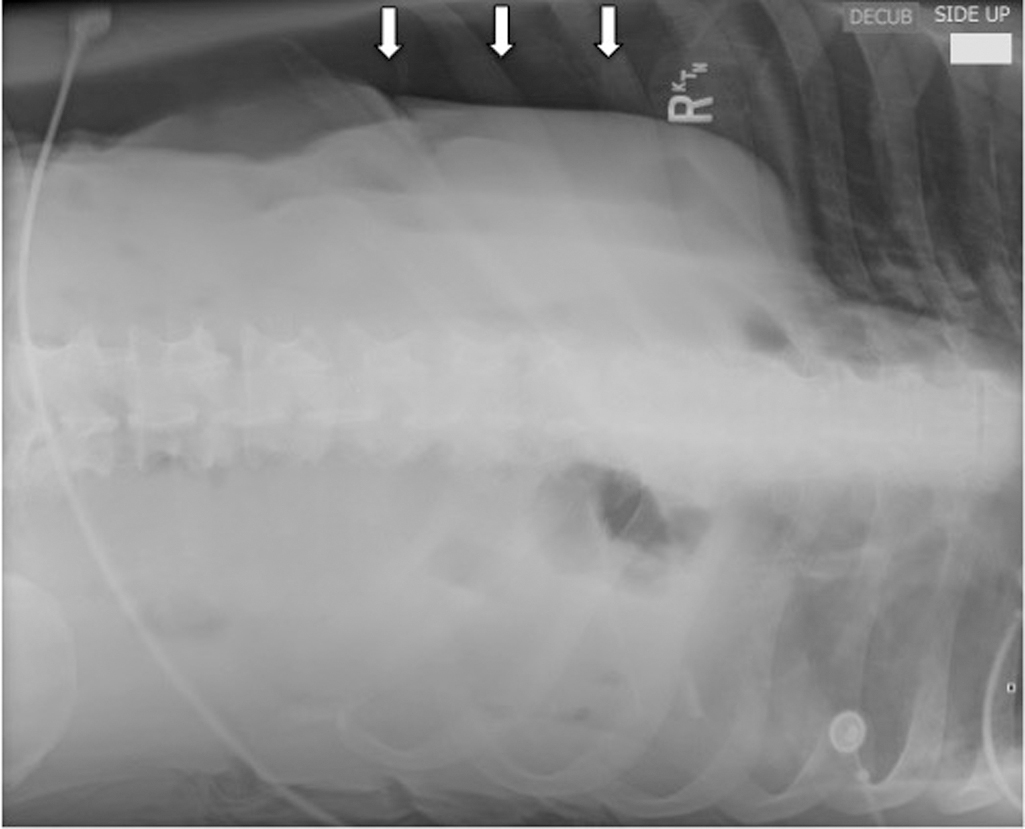
Fig. 4.2
Left lateral decubitus view of the upper abdomen demonstrates free air over the liver ( arrows ).
- ◼
Numerous signs of pneumoperitoneum have been described, including:
- ◼
Rigler’s sign: air seen on both sides of the bowel wall.
- ◼
Falciform ligament sign: air outlining the falciform ligament.
- ◼
Football sign: large amount of air confined to the peritoneal cavity.
- ◼
Doge cap sign: air trapped within Morison’s pouch in the right upper quadrant.
- ◼
Cupola sign: air collecting beneath the central tendon of the diaphragm.
- ◼
Fluoroscopy
- ◼
Provides dynamic evaluation of the GI tract.
- ◼
Extraluminal contrast will not follow the luminal contour, does not peristalse, and may collect dependently.
- ◼
Useful for demonstrating fistulas and communicating collections.
Ultrasound
- ◼
Less commonly performed, but useful as an emergent bedside technique, as well as in pediatric populations.
- ◼
Peritoneal stripe sign: enhancement of the parietal peritoneum because of a highly reflective interface with an antidependent collection of free air.
- ◼
Small echogenic gas bubbles associated with comet tail artifact, ring down artifact, or dirty shadowing.
Computed tomography
- ◼
Highest sensitivity for detection of free air, and allows for thorough evaluation of most possible sources.
- ◼
Computed tomography (CT) detects site of perforation in 85% of cases.
- ◼
- ◼
If perforation is suspected, always review the full series in lung windows.
- ◼
Perforation may be seen on CT enterography, which is often obtained in cases of inflammatory bowel disease and includes the use of larger volume negative oral contrast with intravenous contrast.
Magnetic resonance imaging
- ◼
Although helpful for better tissue characterization and in evaluation of fistula formation, CT is the preferred cross-sectional modality.
- ◼
Magnetic resonance enterography is useful for following patients with chronic inflammatory bowel disease to reduce radiation exposure.
Protocols
Fluoroscopy
- ◼
Any evaluation of suspected hollow viscus perforation should be performed as a single-contrast technique with water-soluble contrast to avoid barium-induced peritonitis.
- ◼
Scout images should be obtained, to serve as a baseline comparison as well as a check for free air. If possible, upright views are preferred.
- ◼
Ideally, enough contrast would be administered to distend the lumen in question; however, this is not always possible in an acutely ill patient.
- ◼
Care should be taken to position the patient so that all mucosal surfaces are evaluated, as small, antidependent disruptions may be missed.
- ◼
When acquiring initial images, cine mode is helpful to better locate the site of disruption.
- ◼
If no leak is found, a thin barium solution may be given to improve contrast.
Computed tomography
- ◼
When possible, an ideal examination includes water-soluble oral contrast and intravenous contrast. However, even a noncontrast examination will demonstrate the presence of free air.
- ◼
CT enterography: the patient should be nothing-by-mouth (NPO) for at least 4 hours before the scan, and instructed to drink 1.5 to 2 liters of neutral or low-density oral contrast over 45 minutes. Single phase supine axial images are obtained 50 seconds after administration of IV contrast (enteric phase) with 2 mm slice thickness and 0.75 mm reconstruction intervals.
- ◼
Some institutions also choose to use antiperistaltic agents, such as glucagon or hyoscine butylbromide.
- ◼
- ◼
Emergent appendicitis protocol: although losing favor, rectal contrast may be given in lieu of oral contrast to reduce the time to scan. Up to 1500 mL of contrast is administered under gravity via rectal tube, with scout imaging confirming that it has reached the cecum. Following injection of IV contrast, thin section axial slices are obtained through the abdomen.
Specific disease processes
Inflammation/infection
Peptic ulcer disease
- ◼
Most common cause of hollow viscus perforation (10% lifetime prevalence with 2%–5% incidence of perforation).
- ◼
More likely within the first portion of the duodenum than stomach.
- ◼
95% of duodenal ulcers occur in the bulb.
- ◼
Most ulcers are <1 cm at time of diagnosis.
- ◼
Marginal ulceration (on the jejunal side of the gastrojejunal anastomosis) following Roux-en-Y gastric bypass occurs on average 1.5 years following surgery in around 1% of patients.
- ◼
- ◼
- ◼
Fluoroscopy
- ◼
See Chapter 3 for evaluation of ulcer disease.
- ◼
In postbulbar ulcers, look for an indentation on the wall opposite the ulcer, representing edema and muscular spasm.
- ◼
- ◼
Computed Tomography
- ◼
Wall-thickening, luminal narrowing, adjacent inflammatory changes.
- ◼
Extravasation of contrast, particularly if on the dependent wall.
- ◼
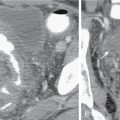
Intraperitoneal predominant air if involving the stomach, and first and fourth portions of the duodenum; retroperitoneal air if second or third portions of the duodenum ( Fig. 4.3 ).
- ◼