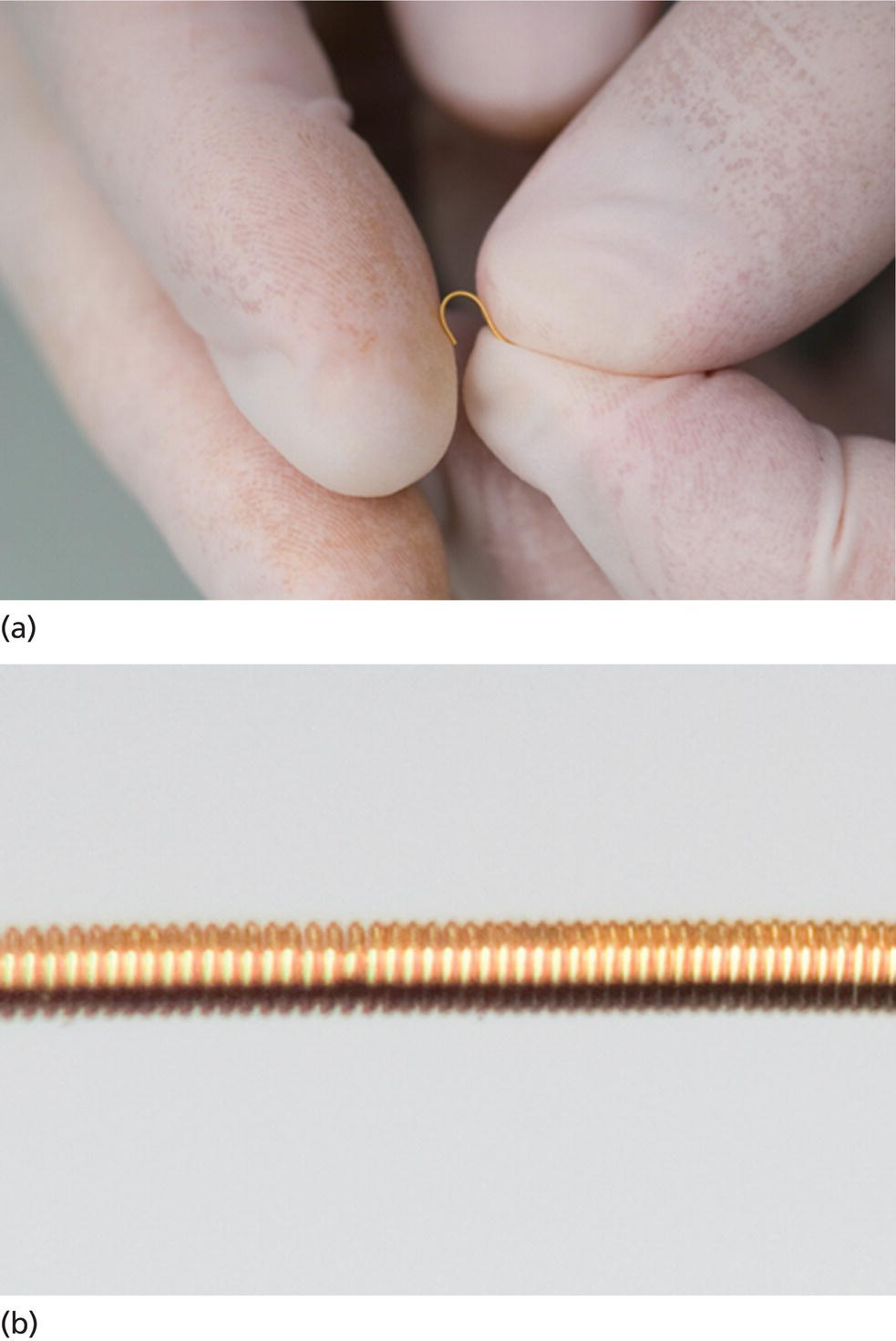
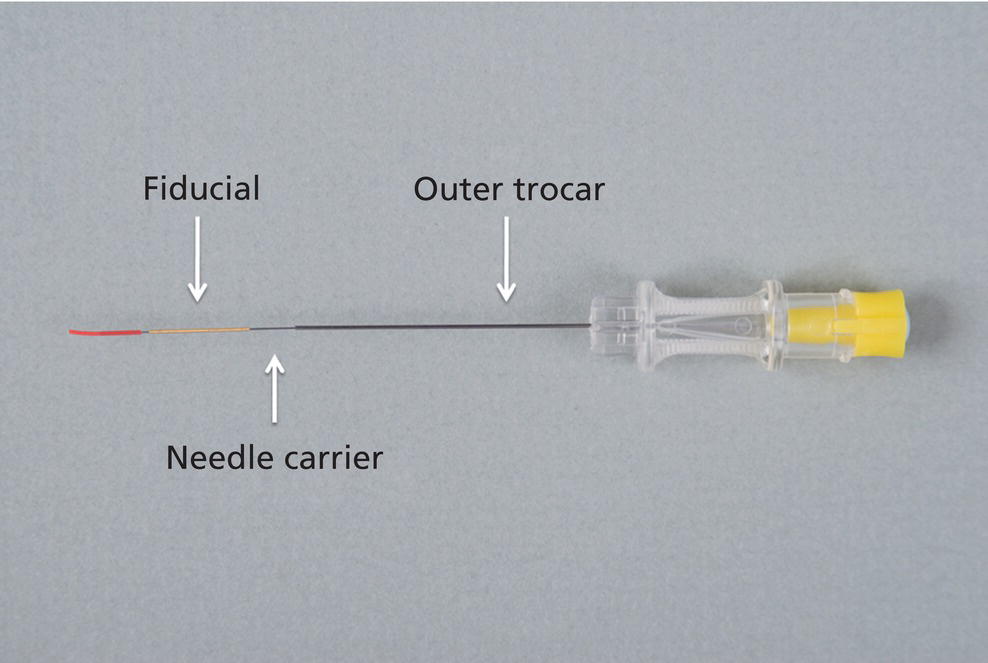
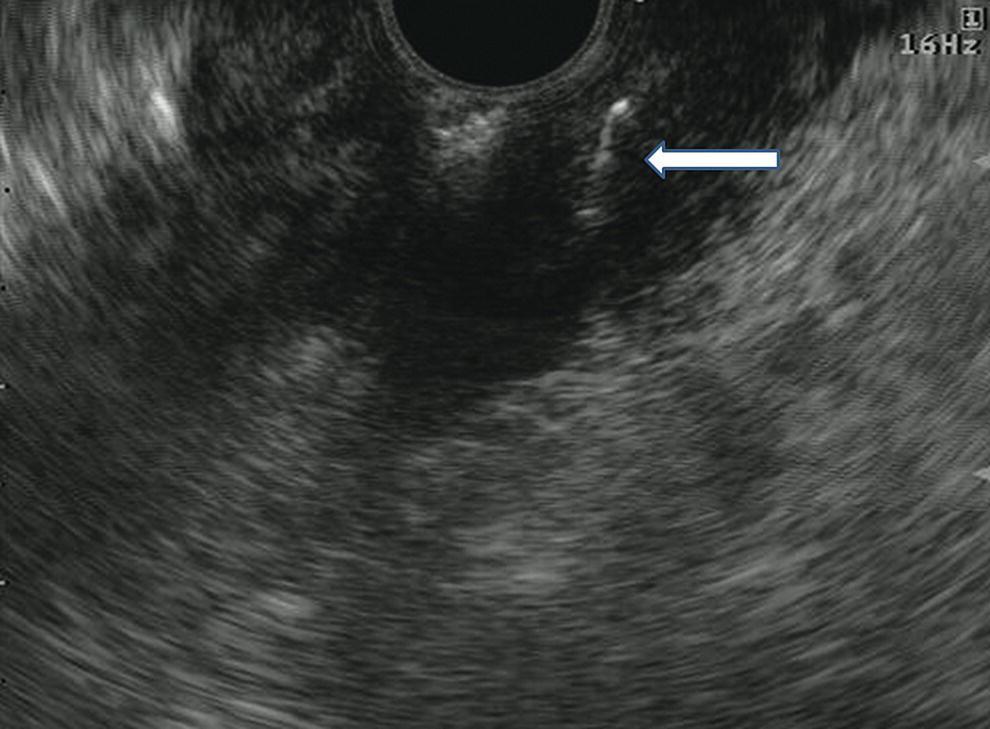
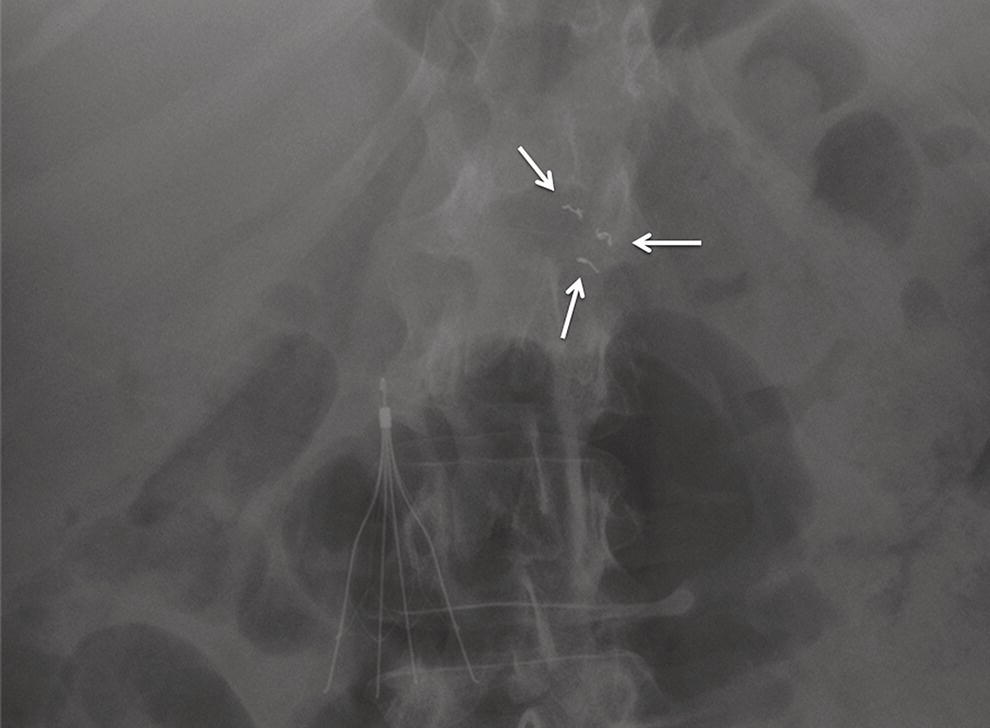
Antonio R. Cheesman, Satish Nagula, and Christopher J. DiMaio Icahn School of Medicine at Mount Sinai, New York, NY, USA Traditional radiation therapy (RT), involving the delivery of high doses of toxic radiation to a target field, is wrought with the unfortunate consequence of acute and chronic injury to healthy tissue adjacent to the tumor. The development of real‐time image‐guided radiation therapy (IGRT) systems allows for the safe delivery of focal high‐dose RT to target lesions while minimizing the amount of collateral damage to normal tissue. These techniques, such as stereotactic radiosurgery and intensity‐modulated RT, allow for the precise delivery of RT by being able to verify the target location and track its movement during the respiratory cycle. IGRT is dependent on reference points by which the target lesion can be identified and tracked. Fiducials are inert radiographic markers which are implanted into the target lesion for this purpose. Given the ability of endoscopic ultrasound (EUS) to allow for close proximity to structures in the mediastinum, abdomen, and pelvis that may not otherwise be accessible by percutaneous approaches, the use of EUS‐guided fiducial placement into both luminal and extraluminal targets has become an accepted technique. Several types of fiducial markers and delivery systems exist. Traditional fiducials are cylindrical gold seeds measuring 3–5 mm in length by 0.75–1.2 mm in diameter, and are deployed using a 19‐gauge fine needle aspiration (FNA) needle. Newer fiducial designs aim to reduce fiducial migration. Coiled fiducials (Visicoil; IBA Dosimetry, Memphis, TN) are flexible gold coil markers measuring 5–30 mm in length by 0.35–1.1 mm in diameter, and are deployed using a needle‐carrier delivery device that fits a 22‐gauge FNA needle. (Figure 36.1 and Video 36.1) Notched fiducials (Gold anchor; Naslund Medical Inc., Chicago, IL) are 10–20 mm in length by 0.28–0.4 mm in diameter, and can be deployed using a 22‐ to 25‐gauge FNA needle. These have notches every 2 mm and can take a linear or circular configuration by withdrawing the needle versus pushing the fiducial forward during deployment. Band fiducials (X‐seed and X‐mark; ONC Solutions Inc., Acton, MA) are 5 mm or 10–30 mm long by 0.85 or 1.15 mm in diameter and consist of separate gold bands overlying a central axle, permitting tissue ingrowth. These fiducials are deployed using 17‐ or 18‐gauge needles and thus may have limited applications for EUS‐guided implantation given the lack of availability of these FNA needle sizes. Multi‐fiducial delivery systems also exist. These include a two 5‐mm long by 0.43–0.75‐mm diameter fiducial system deployed using a 19‐ or 22‐gauge needle (Beacon™ FNF Pre‐loaded Needle; Medtronic, Minneapolis MN) and a four 5‐mm long by 0.43‐mm diameter fiducial system delivered using a 22‐gauge needle (EchoTip® Ultra Fiducial Needle; Cook Medical, Bloomington, IN). Finally, novel radiopaque hydrogel markers (TraceIT Tissue Marker; Augmenix Inc., Bedford, MA) have been designed to fade after three months, and consist of iodinated polyethylene glycol hydrogel particles which can be delivered using a 25‐gauge FNA needle. The available literature suggests traditional fiducials maintain better visibility, newer devices appear to offer limited benefit in migration rates, while wider‐diameter fiducials requiring 19‐gauge needles are associated with limited endoscope angulation resulting in suboptimal target visualization and increased technical failure rates. Fiducials not preloaded on a delivery system can be loaded into EUS needles and deployed using various techniques. The back‐loading, dry deployment method requires withdrawal of the stylet 2–3 cm from the needle tip, back‐loading the fiducial into the needle lumen and sealing the needle tip using bone wax; deployment is performed by advancing the stylet. Otherwise, the back‐loading, hydraulic deployment technique requires complete removal of the stylet, filling the needle channel with sterile water, back‐loading the fiducial into the needle lumen and sealing the needle tip using bone wax; deployment is achieved by injecting 1–2 ml of sterile water through the needle channel. Finally, the back‐loading, wet‐fill method is performed by retracting the stylet while the needle is submerged in sterile water, and back‐loading the fiducial into the needle lumen without the need to seal the needle tip owing to surface tension; deployment is performed by pushing the stylet. Figure 36.1 Gold coil fiducial marker is (a) flexible and (b) has a coiled design. Contrary to the latter techniques, where placement of each fiducial involves needle withdrawal, the push‐stylet technique or front‐loading approach allows for insertion of multiple fiducials without needle withdrawal. This is performed by inserting the needle into the target lesion without a preloaded fiducial, fully withdrawing the stylet, front‐loading the fiducials through the needle handle and advancing them by reinserting the stylet. Finally, coiled fiducials (Figure 36.2 and Videos 36.1 and 36.2), multi‐fiducial delivery systems, and radiopaque hydrogel markers have carrier delivery devices that facilitate loading and deployment. EUS‐guided fiducial placement is performed with standard linear echoendoscopes. Doppler is typically used to identify and avoid vessels in the path of the needle. Once a safe window has been identified, the needle is inserted into the target lesion under EUS guidance (Figure 36.3). Figure 36.2 Gold coil fiducial preloaded on needle‐carrier delivery device. Figure 36.3 Endoscopic ultrasound image (linear array) of fiducial within an adenocarcinoma of the gastroesophageal junction. Figure 36.4 Abdominal radiograph (anteroposterior view) demonstrating three fiducials (arrows) located in an adenocarcinoma of the pancreatic head. The number of fiducials placed is dependent on the size and location of the lesion. For small lesions measuring 1–3 cm (e.g. gastroesophageal junction tumors), a minimum of two fiducials should be placed to define the proximal and distal margins of the tumor. For larger lesions (e.g. pancreatic tumors), three to four fiducials should be placed in varying locations to define tumor borders and planes (Figure 36.4). Different IGRT protocols may call for specific fiducial locations, and thus preprocedure planning with a radiation oncologist is critical. The use of either a sterile or clean non‐sterile technique is acceptable when handling the fiducial markers, EUS needle, and bone wax. Antibiotic prophylaxis is typically administered intraprocedurally to all patients, although the benefit of this practice is unknown. Standard postprocedure monitoring of patients should be performed. Complications related to EUS‐guided fiducial placement are rare, but site‐specific pain and infectious and inflammatory complications have been reported. Fiducial migration into adjacent soft tissue and vascular structures, or even loss into the luminal space, can occur. Treatment‐planning computed tomographic imaging is typically obtained five to seven days after endoscopic placement to confirm fiducial position and relationship to the target lesion.
36
How to Place Fiducials for Radiation Therapy
Introduction
Equipment
Fiducials and needles
Techniques
Fiducial loading and deployment
EUS‐guided fiducial placement (Video 36.3)
Periprocedural care
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


