Key Points
- •
Point-of-care ultrasound is an effective, noninvasive tool to rapidly and accurately assess hemodynamically unstable patients at the bedside.
- •
Hypovolemic, cardiogenic, obstructive, and distributive shock can be readily recognized using established point-of-care ultrasound protocols.
- •
Serial bedside ultrasound exams can be performed to monitor critically ill patients in shock.
In hemodynamically unstable patients, point-of-care ultrasound allows providers to rapidly differentiate the etiology of shock at the bedside and monitor response to therapies. Selecting and delivering life saving interventions to reverse shock is entirely dependent on identifying the underlying etiology; for example, massive fluid resuscitation required in hypovolemic shock would cause immediate decompensation if delivered to a patient with acute cor pulmonale, or inotropic therapy initiated in a volume-depleted patient could likewise end in death. The majority of point-of-care cardiac ultrasound exams in critically ill shock patients consists of five standard assessments that allow for accurate classification and guidance of proper therapy :
- 1.
Left ventricular size and function —presence or absence of regional wall motion abnormalities (RWMA)
- 2.
Right ventricular size and function
- 3.
Pericardial effusion —presence or absence of pericardial effusion
- 4.
Intravascular volume status —IVC diameter and variation, filling of LV and RV
- 5.
Valvular abnormalities —color flow Doppler screening for severe mitral regurgitation
Various published protocols describe a point-of-care ultrasound approach to patients in shock. The five standard assessments described above are the pillars of the goal-directed echocardiography (GDE) approach but are also core components of other shock protocols, such as the RUSH and RACE protocols. The Rapid Ultrasound in Shock (RUSH) protocol combines the same principles of GDE with other diagnostic bedside ultrasound exams. The RUSH protocol includes evaluation of the heart from parasternal long-axis and subcostal 4-chamber views, and the IVC from a subcostal view. In addition, the abdomen, thorax, and lower extremities are examined for peritoneal free fluid, abdominal aortic aneurysm, pleural effusion, pneumothorax, and lower extremity deep venous thrombosis. RACE and other protocols include a similar cardiac evaluation as the GDE and RUSH protocols. The key ultrasound findings to evaluate patients in shock are summarized in Table 40.1 .
| Hypovolemic Shock | Cardiogenic Shock | Obstructive Shock | Distributive Shock | |
|---|---|---|---|---|
| Cardiac exam | LV :
RV :
| LV :
RV :
| LV : Tamponade :
| LV :
RV :
|
| Pulmonary exam | Lungs :
Pleura :
| Lungs :
Pleura :
| Lungs :
| Lungs :
|
| IVC exam | Collapsed IVC | Distended IVC | Distended IVC | Normal/collapsed IVC |
| Supplementary exams | Abdomen :
| Abdomen :
| Vascular :
| Abdomen :
|
Case Studies
Case Presentation
A 59-year-old man with a past medical history of coronary artery disease and myocardial infarction presented to the emergency department with lightheadedness and near syncope. Vital signs: temperature 38 °C, pulse 122 bpm, blood pressure 86/40 mm Hg, respiratory rate 28/min, oxygen saturation 88%.
Physical exam: Fatigued appearance, lethargic, moderate respiratory distress, dry mucous membranes, unable to complete full sentences, tachycardic without murmur, faint crackles in bilateral bases, no peripheral edema.
Initial testing was significant for leukocytosis, elevated lactate, and pyuria on urinalysis. Chest x-ray revealed bilateral interstitial opacities with an oxygen saturation of 88% on a 100% non-rebreather mask. ECG revealed an old left bundle branch block. Initial troponin was normal.
Assessment
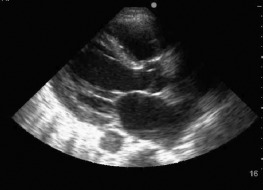
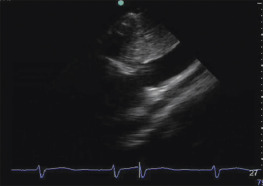
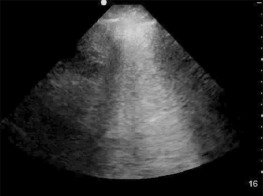
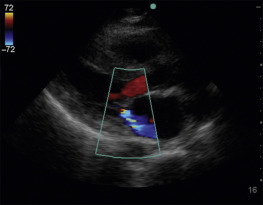
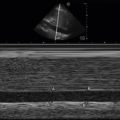
Sepsis was suspected as the underlying cause of patient’s hypotension and lethargy based on presence of fever and pyuria. The chest radiograph was attributed to development of acute respiratory distress syndrome given the patient’s volume depletion without peripheral edema. Intravenous fluid resuscitation was initiated, but neither blood pressure nor clinical exam improved after 2 L of intravenous fluids. The critical care team was consulted and performed a focused cardiac and lung ultrasound exam that revealed the following ( Figures 40.1 to 40.4 and ![]()
![]()
![]()
![]() ):
):
- ▪
Left ventricle (LV) size and function: LV dilated with severely reduced function (reduced endocardial excursion, reduced myocardial thickening, and limited septal motion of the anterior leaflet of the mitral valve).
- ▪
Right ventricle (RV) size and function: Limited assessment, RV seen only in parasternal long-axis view; however, appears slightly enlarged, possibly hypocontractile in this view.
- ▪
IVC size and collapsibility: Dilated to almost 3 cm, noncollapsible.
- ▪
Pericardial effusion: Absent.
- ▪
Valvular function: Moderate MR seen on color flow Doppler.
- ▪
Lung ultrasound: Anterior lung points significant for confluent B-lines with smooth, thin pleura that is sliding
The severely reduced global LV function suggested a possible primary cardiac cause of hypoperfusion. The bilateral anterior lung points with confluent B-lines and smooth, thin, sliding pleural line is consistent with hydrostatic pulmonary edema with a pulmonary artery occlusion pressure greater than 18 mm Hg. The dilated IVC provides further evidence of increased cardiac filling pressures. Absence of severe mitral regurgitation confirmed acute cardiogenic shock from LV failure as the primary cause. Dobutamine infusion, diuresis, and anticoagulation were initiated with improvement in dyspnea, urine output, and mental status. Repeat troponin was elevated, and urgent cardiac angiography revealed an occluded left anterior descending artery that was treated with angioplasty and stent placement.
Case Resolution
Cardiogenic shock presents with signs of a low cardiac output state, usually presenting with oliguria, cool extremities, decreased mental status, and hydrostatic pulmonary edema. Patients without a previous history of congestive heart failure warrant further investigation for an acute inciting event. The treatment of cardiogenic shock should be directed at reversing the underlying cause, most commonly ischemia, infarction, or acute on chronic left ventricular failure. Diuretic and/or inotropic therapy with dobutamine should be initiated to support perfusion. Response to therapy can be confirmed and monitored noninvasively with improvement in clinical findings such as urine output or with serial repeat bedside ultrasound exams showing improved LV systolic function and decrease in interstitial pulmonary edema.
Case Pearls
- ▪
The presence of bilateral, B-line patterns without sparing in the anterior lung exam points and a thin, smooth, sliding pleura is diagnostic of hydrostatic pulmonary edema.
- ▪
Color flow Doppler screening of the mitral valve for severe mitral regurgitation should be performed in any patient with hydrostatic pulmonary edema and shock.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


