CHAPTER 31 Imaging of Atrial Fibrillation Intervention
DEFINITION
AF, a supraventricular tachyarrhythmia, is the most common cardiac arrhythmia with an overall prevalence of 0.4% to 1%.1 AF manifests clinically with an “irregularly irregular” heart rate, lack of P waves on ECG, and heart rates of up to 200 beats/min. To guide treatment options, the American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC) has issued guidelines classifying AF into paroxysmal, persistent, and permanent.2 Paroxysmal AF is defined as AF lasting less than 7 days and terminating spontaneously. Persistent AF lasts longer than 7 days and requires cardioversion to achieve normal sinus rhythm. Permanent AF lasts longer than 1 year. When AF occurs in individuals younger than 60 years and without underlying risk factors, it is termed lone AF.
PREVALENCE AND EPIDEMIOLOGY
AF affects approximately 2.3 million people in the United States and more than 6 million people in Europe.3 Its prevalence increases with age. Although AF is rare in children, in adults, the incidence and prevalence double every 10 years after age 50. The lifetime risk of developing AF is one in four after age 40.
Epidemiologic studies have linked AF to underlying structural heart disease, particularly mitral valvular disease, hypertension, and coronary artery disease.4 Age, diabetes, smoking, obesity, male sex, and white race are also independently associated with increased risk of AF.1,2 The epidemics of obesity and chronic heart failure are expected to contribute to an increased incidence of AF. The total annual cost for treatment of AF is estimated at $6.65 billion.5 AF results in approximately 350,000 hospitalizations, 5 million office visits, and 276,000 emergency department visits annually in the United States.
PATHOPHYSIOLOGY OF ATRIAL FIBRILLATION AND PULMONARY VEINS
The pathophysiology of AF is complex and not fully understood. AF is initiated by rapid firing of ectopic foci or re-entrant wavelets most often (94%) originating from the pulmonary veins.6 Other sources of ectopic foci have been identified in superior vena cava, coronary sinus, ligament of Marshal, crista terminalis, body of left atrium and right atrium, and more distal pulmonary veins.7–9 Pathologic studies have shown the extension of myocardial sleeves into pulmonary veins.10 A sleeve of myocardium surrounds the proximal aspect of the pulmonary vein and when measured from the venoatrial junction extends 0.2 to 1.7 cm out of the pulmonary veins with the longest sleeves associated with the superior pulmonary veins. The longest extensions occur in the following order: left superior pulmonary vein, right superior pulmonary vein, left inferior pulmonary vein, and right inferior pulmonary vein.11 Haissaguerre and colleagues6 showed a similar rank order when identifying ectopic foci for ablation. More than 90% of these ectopic beats arise from pulmonary veins; 50% arise from the left superior pulmonary vein alone. The posterior left atrium and pulmonary veins have become the focus of attention in treatment efforts of AF. When initiated, an abnormal atrial substrate maintains AF in susceptible individuals. Current AF treatments strive to isolate electrically the originating foci in the pulmonary veins from the atrial substrate and to modify the substrate.
MANIFESTATIONS OF DISEASE
Clinical Presentation
AF prevents ventricular preload and is associated with increased cardiovascular morbidity or mortality.12 It is an independent risk factor for stroke, increasing the risk by threefold to fivefold.4,13 It is also associated with increased risk of systemic embolism. The source of the embolism is left atrial appendage (LAA) in most patients.14 AF is associated with an increase in overall mortality in multiple studies.15,16
Clinically Relevant Anatomy
The left atrium can be divided into four components: the septum, the vestibule, the appendage, and the venous portion. The walls of the left atrium are described as superior, posterior, left lateral, septal, and anterior.17 The anterior wall behind the transverse pericardial sinus posterior to the aorta is very thin, averaging 2 mm in thickness.18 The thickest portion of the left atrium is the superior wall, averaging 4.5 ± 0.6 mm in thickness.18
The interatrial septum comprises the foramen ovale. The foramen ovale is a flap valve that typically fuses by early adulthood. The prevalence of patent foramen ovale is reported to be 25%.19 The foramen ovale is the only portion of the septum that can be traversed without risk of injury to the sinoatrial nodal artery or exiting the heart.18
Most of the left atrium is smooth-walled. The exception is the LAA, which is derived from the primitive atrium and contains multiple pectinate muscles and a trabeculated surface. The LAA is a common source of atrial thrombi because of relative stasis of blood flow in this region in AF and the narrow neck of the appendage. Accessory atrial appendages (also termed roof pouch) have been reported in 0.06% of patients; these are of unclear clinical significance, but they may result in discontinuity of a roof ablation line if unrecognized (Fig. 31-1).20,21
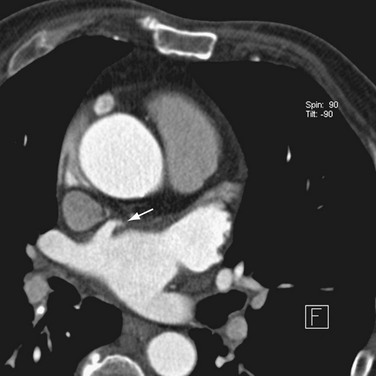
 FIGURE 31-1 Accessory LAA. A focal outpouching (arrow) is seen anterior to the right superior pulmonary vein.
FIGURE 31-1 Accessory LAA. A focal outpouching (arrow) is seen anterior to the right superior pulmonary vein.
The venous component comprises most of the left atrium. Classic left atrial anatomy consists of bilateral superior and inferior pulmonary veins and is present about two thirds of the time (Fig. 31-2).22,23 Accessory pulmonary veins are named for the lobes or segments they drain. Common anatomic variants include a conjoined left pulmonary trunk, which bifurcates to form the left superior pulmonary vein and left inferior pulmonary vein (under incorporation) and has been reported as a consistent source of arrhythmogenic atrial ectopy (Fig. 31-3).24,25 An accessory right middle pulmonary vein is the most common variant, occurring 20% to 30% of the time; it originates from the intervenous saddle and is typically 1 cm or less in diameter (Fig. 31-4).26 The next most common accessory vein drains the superior segment of the right lower lobe independently. One of the most striking accessory veins is the “top vein” (3%), which can drain the posterior segment right upper lobe or superior segment right lower lobe, and is particularly important to describe for patients being considered for the Wolf mini-Maze procedure; this unusual location is blind to the thoracoscopist (Fig. 31-5).27,28 Overincorporation of the right inferior pulmonary vein commonly results in multiple orificial branches and has been reported in 66% to 99% of cases (Fig. 31-6).29 Rarely, the inferior pulmonary veins can be conjoined resulting in an inferior truncus (Fig. 31-7).30

 FIGURE 31-2
FIGURE 31-2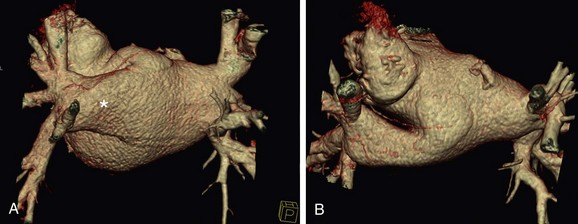
 FIGURE 31-3
FIGURE 31-3
 FIGURE 31-4
FIGURE 31-4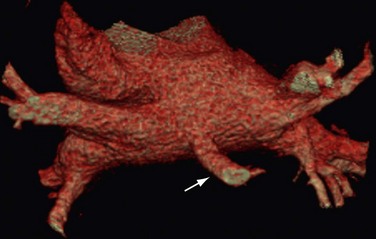
 FIGURE 31-5
FIGURE 31-5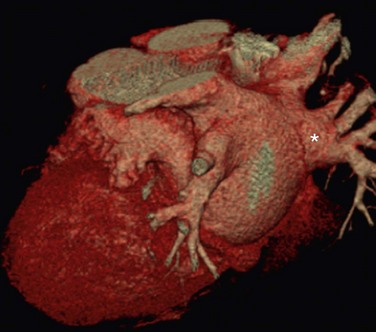
 FIGURE 31-6
FIGURE 31-6
 FIGURE 31-7
FIGURE 31-7The sinoatrial node is found along the course of the sinoatrial artery in the subepicardium. This subepicardial location makes the node more vulnerable to select cardiac surgery and pericardial disease.31 The node artery arises from the right coronary artery in 66% of cases, arises from the left circumflex artery in 27%, and has a dual supply in 6%.32 Most arise from the proximal right coronary artery and course along the anterior interatrial groove toward the cavoatrial junction (Figs. 31-8 and 31-9).

 FIGURE 31-8
FIGURE 31-8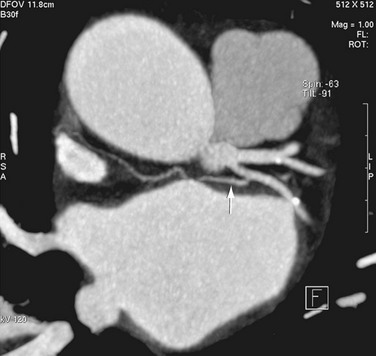
 FIGURE 31-9
FIGURE 31-9CLINICAL TREATMENT OF ATRIAL FIBRILLATION
Traditionally, treatment of AF has included electrical or chemical cardioversion followed by long-term antiarrhythmic therapy. This strategy is unsatisfactory in maintenance of sinus rhythm, with less than 50% of patients being in sinus rhythm after 1 to 2 years.33 It also has the accompanying disadvantage of requiring lifelong anticoagulation. Maintenance of sinus rhythm is important in younger active individuals to decrease the incidence of stroke, and in older patients with heart failure, the loss of the “atrial kick” affects overall cardiac output.
In an effort to improve treatment efficacy, a surgical procedure called the Cox Maze procedure was developed; this procedure results in isolation of the pulmonary veins and compartmentalization of the atria.34 Multiple incisions in both atria result in scar tissue that reduces the amount of atrial tissue between scars to below the critical re-entry circuit size, preventing AF. A thoracoscopic variant of this procedure, the Wolf mini-Maze, was developed in an effort to prevent the more morbid median sternotomy necessitated by the Cox-Maze procedure.35 It is a bilateral video-assisted thoracoscopic off-pump procedure. A curved bipolar radiofrequency (RF) ablation device is used to create bilateral, transmural, linear lesions around an atrial cuff of the right and left pulmonary veins achieving electrical isolation (Fig. 31-10). In addition, a staple excision of the LAA is performed. Relevant to the Wolf mini-Maze procedure, the surgeon is “blind” to the anatomy of the posterior wall of the left atrium. Accessory veins in this region are particularly vulnerable to surgical mishap.28
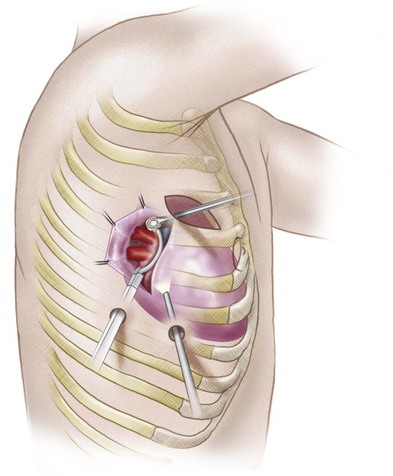
 FIGURE 31-10
FIGURE 31-10Catheter-based procedures have been developed that aim at treating the triggers and the substrate for the AF. Ablation involves the purposeful devitalization of arrhythmogenic myocardial tissue to treat arrhythmias. This devitalization may be accomplished using cryotherapy or, more commonly, RF current to induce a thermal injury. RF lesions are typically 3 to 6 mm in diameter and 3 mm deep.36 More recently, use of externally irrigated catheters has increased in an effort to improve lesion delivery and reduce char formation at the catheter tip, which decreases thermal efficiency.37 The choice of catheter and energy delivery varies among different centers with an emphasis on smaller, lower energy systems. The most recent ACC/AHA/ESC guideline recommends ablation of AF in symptomatic patients who have not responded to medical therapy.2,38 Currently, ablation is performed in a wider array of patients, however, particularly in patients with congestive heart failure, in whom ablation of AF has been shown to improve ventricular systolic function.39
The first contemporary approach to AF ablation was performed by Haissaguerre and colleagues6 in 1994 by point ablation of distal pulmonary vein foci. This procedure was moderately successful, although it was complicated by a high percentage of pulmonary vein stenosis. Since then, multiple approaches have been developed, including segmental isolation of pulmonary veins and circumferential ablation, a stepwise approach that requires additional ablation lines in the roof of the left atrium, mitral annulus and isthmus, and coronary sinus and isolation of the superior vena cava (Fig. 31-11). Ablation of continuous atrial fractionated signals and autonomic ganglia around the pulmonary veins has also been tried.38,40–43 The most common technique includes isolation of pulmonary veins using a circumferential extraostial ablation 1 to 2 cm on the atrial side of the pulmonary veins and isolation of the posterior left atrium.38,44,45 Additional ablation lines may be created in the posterior left atrium, termed the roof ablation line, and at the mitral isthmus.
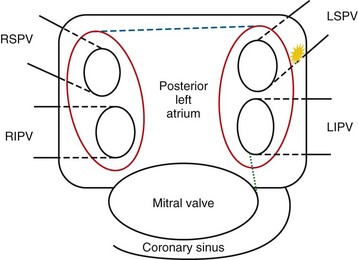
 FIGURE 31-11
FIGURE 31-11Left atrium function is partially preserved with the surgical Maze procedure.46,47 With catheter ablation techniques targeting the posterior left atrium, the pulmonary vein orifices, and the mitral isthmus line, 30% to 40% of left atrial surface area may be ablated.48 Multidetector CT evaluation of left atrial transport after circumferential RF ablation of paroxysmal AF found a decrease in left atrium function, although it is unclear whether this impairment is severe enough to predispose to thrombus formation.49 More recently, Takahashi and coworkers45 reported recovery of left atrium function with stepwise catheter ablation for chronic AF. Patient selection may also be important because pulmonary vein electrical isolation has been shown to be more effective in paroxysmal than in persistent AF.50
Imaging Techniques
The anatomy of the pulmonary veins can be delineated during the procedure by retrograde contrast venography in conjunction with intracardiac ultrasonography.51 More often, a CT or MRI examination of the left atrium is performed before the procedure.52



