Imaging of Cerebral Infection with PET
Alfred Buck
Ehab M. Kamel
T here are a few clear indications for fluorine 18 (18F) fluorodeoxyglucose (FDG)-PET in infectious brain diseases. With MRI and CT, it is sometimes difficult to distinguish between a brain abscess and tumor, especially if the latter is necrotic. FDG-PET may be helpful in this area. Usually the FDG accumulation in the abscess wall is between the level in white matter and the level in gray matter. Unfortunately, this is also the range of the accumulation in some tumors, which limits the usefulness of FDG. If, however, the FDG uptake exceeds that in gray matter, a tumor is much more likely. A promising tracer for differentiating abscess from tumor is [18F]ethyltyrosine, which is not taken up by inflammatory cells.
FDG-PET is very useful for distinguishing between toxoplasmosis and lymphoma in HIV patients. In lymphoma, FDG uptake is above, in toxoplasmosis below, cortex FDG uptake. An example is shown in Figure 24.5.
Introduction
Cross-sectional neuroimaging techniques are very sensitive to any intracerebral alterations. With the clinical history, physical examination, laboratory results, and appearance on CT or MR images, the differential diagnosis between the different disease entities can usually be narrowed down. Because epidural and subdural infections usually do not produce problems in differentiating them from other noninfectious diseases, only intraparenchymal lesions will be discussed in this chapter.
The major point of interest is the differential diagnosis between a primary intracerebral neoplasm and an inflammatory or infectious lesion, mainly an abscess. High-grade tumors (WHO grades III and IV) usually are separated from other intracerebral lesions by their high uptake of fluorine 18 (18F) fluorodeoxyglucose (FDG) when compared with cortical gray matter. This is specially true for anaplastic astrocytomas grade III, glioblastomas, meningiomas, lymphomas, some metastases, and juvenile primary brain tumors. However, difficulties have been described in differentiating even high-grade lesions from granulomatous tissue, especially in ongoing radiation-induced necrosis. It is known from experimental studies (1,2,3) that inflammatory cells do accumulate FDG to a higher degree; therefore, some sort of quantification is usually recommended to help in the differential diagnosis. Another problem is making a differential diagnosis between low-grade tumors and inflammatory or infectious lesions by FDG-PET, since all these lesions exhibit a similar level of FDG uptake. As discussed below, a new promising tracer is [18F]ethyltyrosine, which does accumulate in tumors but not infectious tissue (3).
Pyogenic Brain Abscess
A pyogenic brain abscess is formed through hematogenous dissemination of a primary site. It occurs most often in patients with pulmonary or cardiac infections, patients with infections from the paranasal sinuses, septic patients, and patients with intravenous drug abuse. The brain abscess favors the frontal and parietal lobes along the supplied territory of the middle cerebral artery. It is usually located at the junction of gray and white matter and may occur as a single lesion or as multiple lesions.
Neuroimaging with CT and MRI
Using experimental CT imaging, four stages of abscess formation have been described: (a) early cerebritis (1 to 3 days),
(b) late cerebritis (4 to 9 days), (c) early capsule formation (10 to 13 days), and (d) late capsule formation (14 days and later) (4). In the cerebritis phase, a lesion of low density and patchy enhancement may be seen. In the late cerebritis phase, a necrotic center is formed within the infectious lesion and surrounded by a granulation tissue. Therefore, ring-like enhancement is often present. The mature abscess appears of low density, with considerable edema surrounding the lesion.
(b) late cerebritis (4 to 9 days), (c) early capsule formation (10 to 13 days), and (d) late capsule formation (14 days and later) (4). In the cerebritis phase, a lesion of low density and patchy enhancement may be seen. In the late cerebritis phase, a necrotic center is formed within the infectious lesion and surrounded by a granulation tissue. Therefore, ring-like enhancement is often present. The mature abscess appears of low density, with considerable edema surrounding the lesion.
On magnetic resonance (MR) imaging, the lesion is of low intensity on T1-weighted images and of high signal on T2-weighted images in the early cerebritis phase. After 2 to 3 weeks, the mature abscess appears, as a well demarcated mass of low intensity on T1-weighted sequences, with edema beyond the lesion. On T2-weighted images, high intensity is seen in the cavity.
As ring-like enhancement is seen in the mature abscess on both CT and MR imaging, several differential diagnoses have to be considered, including infarction, fungal or parasitic infection, primary or metastatic brain tumor, tuberculosis, granuloma, multiple sclerosis, and subacute hematoma. In this clinical setting, FDG-PET, in conjunction with conventional neuroimaging, might help in narrowing down the differential diagnosis.
PET with FDG and [18F]Ethyltyrosine
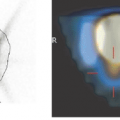
As pyogenic abscesses are surrounded by granulomatous tissue in the late phase of cerebritis, ring-like FDG uptake might be observed (Fig. 24.1). However, this FDG uptake in the granulomatous tissue is inconsistent, and can be missing altogether. This feature is probably dependent on the time of scanning, the amount and the characteristics of the inflammatory cells. It is therefore often difficult to separate tumor and abscess. Glioblastomas are often necrotic and there may be only little tumorous tissue at the edge. In these cases the actual FDG uptake may be underestimated due to the limited resolution of the PET scanner. In such cases an additional PET using an amino acid analogue such as 18F-ethyltyrosine (FET) may be helpful. We demonstrated, that FET is not taken up in experimental abscesses induced in rat muscle (3). Based on this result one can hypothesize that lacking FET uptake would also characterize a brain abscess. In contrast, there is high FET accumulation in brain tumors, as is demonstrated in Figure 24.2.
Related posts:
 PET Radiopharmaceuticals: Perfusion Compounds [13N]Ammonia, [15O]Water, [82RB]Rubidium, and Other Generator Products of Clinical Relevance
PET Radiopharmaceuticals: Perfusion Compounds [13N]Ammonia, [15O]Water, [82RB]Rubidium, and Other Generator Products of Clinical Relevance
 The Normal Brain Scan
The Normal Brain Scan
 Sentinel Node Imaging in Head and Neck Tumors
Sentinel Node Imaging in Head and Neck Tumors
 PET-CT and SPECT-CT of Bone Metastases
PET-CT and SPECT-CT of Bone Metastases
 SPECT and PET in Benign Thyroid and Parathyroid Disease
SPECT and PET in Benign Thyroid and Parathyroid Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


