Masticator space is a paired deep fascial space seen in relation to the ramus of the mandible and may be affected by a myriad of pathologies. Knowledge of its anatomy and contents with characteristic imaging features of each pathology will help to accurately evaluate abnormalities at this site.
Anatomy
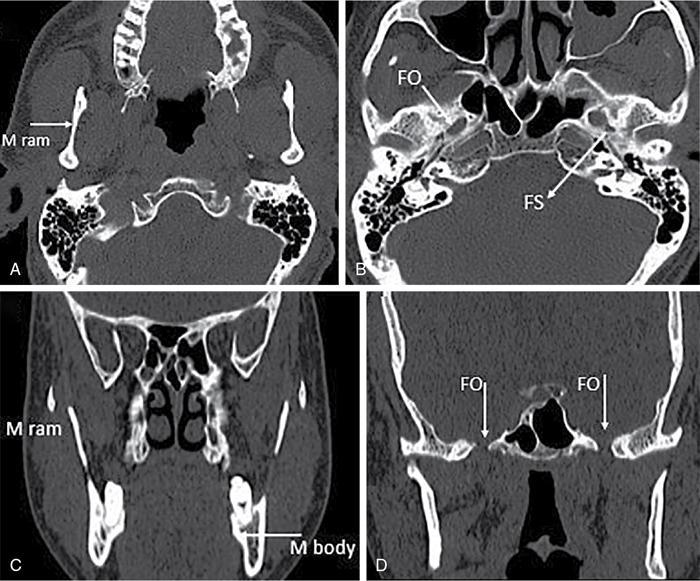
The masticator space (MS) is a deep space seen on either side of midline enclosed by the superficial layer of deep cervical fascia (SL-DCF), which splits at the inferior margin of the mandible (Fig. 3.17.1.1A). The medial slip of SL-DCF, also known as the medial pterygoid fascia, runs along the medial surface of pterygoid muscles and inserts on the undersurface of the skull base medial to foramen ovale. Hence a large part of skull base including foramen ovale and spinosum is included within the MS. On the lateral aspect, the lateral slip of SL-DCF runs over the masseter muscle, attaches to the zygomatic arch and then continues superiorly over the surface of the temporalis muscle (Fig. 3.17.1.1B). The upward extent of the space therefore extends up to the parietal calvarium, The zygomatic arch divides the MS into suprazygomatic and infrazygomatic (or nasopharyngeal) portions.
Fig. 3.17.1.1Masticator space outlined in axial (A) and coronal (B) CT using soft-tissue algorithm identifying normal contents of MS. LP, lateral pterygoid muscle; M, masseter muscle; MP, medial pterygoid muscle; T, temporalis muscle.
Relations
Buccal space is anterior to MS, and parotid space is posterolateral to MS. Parapharyngeal space is medial to MS.
Contents of masticator space
1. Muscles of mastication (masseter, temporalis, medial and lateral pterygoid muscles)
2. Mandibular body and ramus
3. Mandibular division of trigeminal nerve (CN 5)
4. Inferior alveolar nerve, artery and vein
5. Pterygoid venous plexus
The mandibular body and ramus are the osseous components of the space (Fig. 3.17.1.2A and C). The muscles of mastication include the masseter, temporalis, medial and lateral pterygoid muscles (Fig. 3.17.1.1A–B). Masseter is the principle and strongest muscle of mastication. Lateral pterygoid is the primary abductor (jaw opener) of the jaw, while the rest are adductors (jaw closers). The mandibular division of the trigeminal nerve (V3) enters the MS space via the foramen ovale (Fig. 3.17.1.2B and D). Inferior alveolar nerve, a branch of V3, enters the mandibular foramen to run within the inferior alveolar canal along with the inferior alveolar artery and vein. Pterygoid venous plexus is a cluster of venules in the medial masticator and parapharyngeal space around the pterygoid and temporalis muscles, especially bearing a close relationship with the lateral pterygoid muscle. Pterygoid plexus drains into maxillary vein, which joins the superficial temporal vein to form the retromandibular vein.
Fig. 3.17.1.2Axial (A,B) and coronal (C,D) CT using bone algorithm shows FO, foramen ovale; FS, foramen spinosum; M body, body of mandible; M ram, Ramus of mandible.
Pathology of masticator space
Vascular anomalies
• Vasoproliferative lesions
• Infantile haemangioma
• Congenital haemangioma
• Vascular malformations
• Venous malformations
• Lymphatic malformation
• Arteriovenous malformation
• Combined
Infective/inflammatory
• Phlegmon/cellulitis/abscess
• Atypical infections/inflammation
• Fungal/tubercular/actinomycosis/parasitic
• Granulomatous polyangitis
Benign tumours
• Neural origin
• Schwannoma
• Neurofibroma
• Bony origin
• Odontogenic/nonodontogenic jaw cysts and tumours
• Soft-tissue tumours
• Lipoma
• Rhabdomyoma
Malignant tumours
• Intrinsic
• Osteosarcoma
• Chondrosarcoma
• Rhabdomyosarcoma
• Non-Hodgkin’s lymphoma
• Extrinsic
• Extension of malignancy from parotid, oral cavity, nasopharynx
• Perineural spread along V3
Miscellaneous/pseudolesions
• Masticator muscle hypertrophy
• Asymmetric pterygoid venous plexus
• V3 denervation atrophy
• Accessory parotid gland
General features of masticator space pathology
• Pathology of masticator space is centred in muscles of mastication/mandibular ramus. The parapharyngeal fat is displaced posteromedially by pathology in masticator space.
• In pathology of MS, the cephalad extent must be ascertained over the parietal calvarium to delineate the entire extent. Coronal plane is the best plane to evaluate the suprazygomatic extent of the pathology.
Imaging modalities in MS pathology
• Both CT and MR can be used to assess the masticator space. CT is the modality of choice for infectious pathology as underlying bone changes can be easily appreciated on CT. Both soft tissue and bone algorithm must be evaluated to look for soft-tissue changes as well as underlying osteomyelitis and dental caries.
• MR is the preferred modality in suspected neoplasm as it has superior soft-tissue resolution, depicts marrow invasion better and is the most sensitive tool to detect perineural spread.
• Ultrasound (US) has severe limitations in evaluation of head and neck masses owing to presence of bone and air, which hamper visualization of deeper compartments of neck; however, it can be used as an initial modality to evaluate nature of any superficial mass, especially in paediatric patients. US also plays a major role in evaluation of vascular anomalies of MS and to safely guide needle biopsies of masses that can be visualized by ultrasound.
Imaging features of common pathologies
Vascular anomalies
Vascular anomalies can be broadly classified into haemangiomas and vascular malformations. These are dealt with briefly here and discussed in detail in the chapter on “vascular lesions”. Imaging plays a pivotal role in identifying and characterizing the vascular lesions. Another key role of imaging is in defining the extent of the lesion.
• Infantile haemangioma is a true benign vascular neoplasm and is the most common benign neoplasm of masticator space in the paediatric age group. It usually presents shortly after birth, then grows in its proliferative phase and involutes by the age of 10 years. On MRI, it is commonly seen as a well-defined, slightly lobulated soft-tissue mass appearing hypointense on T1-weighted and hyperintense on T2-weighted images. It characteristically shows intense enhancement following gadolinium injection.
• Vascular malformations are another set of vascular anomalies present since birth, but unlike haemangiomas they continue to grow and do not involute as the child ages. They are further classified on the basis of their flow characteristics as slow flow vascular malformations (venous malformations, lymphatic malformations, venolymphatic malformations) and high flow vascular malformations (arteriovenous malformations).
Venous malformation
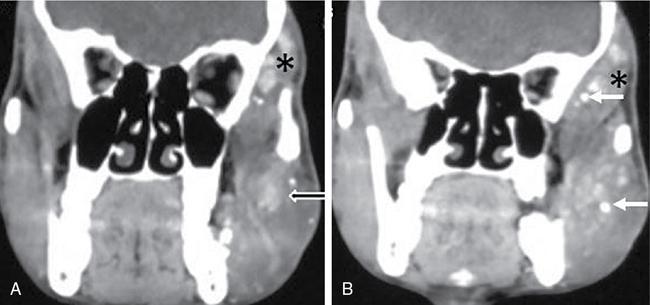
It is a type of slow flow vascular malformations which is commonly seen to involve the masseter muscle in the MS. It can appear as an infiltrative lesion that extends into adjacent muscles and the mandible. For a superficial lesion, USG with Doppler (colour and spectral) evaluation can be the initial imaging modality of investigation. On USG, these are seen as multiloculated cystic masses with internal debris. These are often transspatial, and although ultrasound identifies the lesion, its entire extent and anatomical correlation is accurately determined by cross-sectional imaging (CT, MRI). On CT, it is seen as a hypodense mass relative to the muscle (Fig. 3.17.1.3A) with slow enhancement following contrast injection. On MRI, it is typically hypointense on T1-weighted, hyperintense on T2-weighted images with significant heterogenous enhancement following gadolinium injection. Presence of calcific foci representative of phleboliths is hallmark for venous malformation (Fig. 3.17.1.3B), and they are seen as focal curvilinear hyperechoic areas with posterior acoustic shadowing on USG, hyperdense foci on CT and as signal voids on MRI.
Fig. 3.17.1.3Masticator space venous malformation. In an 18 year-old male with painless left facial swelling, CECT coronal (A,B) shows an ill-defined heterogeneously enhancing soft-tissue lesion ( black arrow with white outline) in the left masticator space with suprazygomatic extension ( star). The lesion shows multiple calcific foci within ( white arrows) representing phleboliths characteristic of venous malformation.
Lymphatic malformation
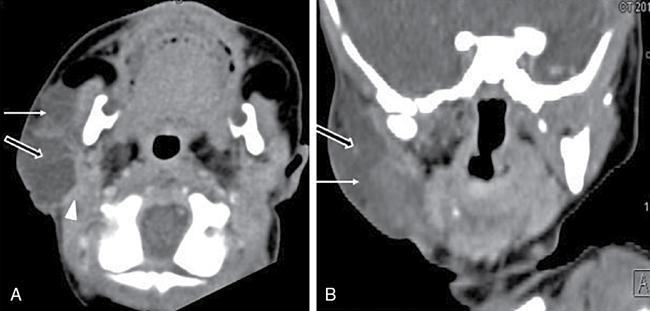
Lymphatic malformations can be divided into two types, namely, microcystic and macrocystic, based on their imaging appearance. Microcystic lesion is composed of many small cysts with internal septations and are mainly seen as infiltrative solid lesions with little fluid on imaging, whereas macrocystic lesion is composed of large cysts with fewer septations. On CT imaging, the macrocystic variety is seen as a multiloculated hypodense mass (Fig. 3.17.1.4A and B). On MRI, signal intensity is variable depending on the presence of haemorrhagic and proteinaceous content within. Multiple “fluid–fluid levels” seen due to repeated haemorrhage within the lesion are characteristic of a lymphatic malformation. The walls and internal septations enhance on postcontrast images.
Fig. 3.17.1.4Masticator space lymphangioma. In a 1-year-old child, axial (A), coronal (B) CECT images show a well-defined multiloculated cystic lesion ( white arrow) with enhancing internal septations ( black arrow with white outline) in right masticator and parotid space ( white arrow head).
Arteriovenous malformation
Arteriovenous malformation (AVM) is high flow vascular malformation, i.e. it has an arterial component. It may be confined to the soft tissues or be intraosseous in location, involving the mandible. Patients present with cheek swelling, discoloration of overlying skin and facial asymmetry. On USG Doppler evaluation, presence of arterial pattern of waveform is seen in the vascular channels. On MRI, presence of multiple dilated serpiginous vascular channels with little or no soft tissue is typical for AVM. These vascular channels are seen as flow voids on all sequences. Identification of feeding arteries and draining veins is important to plan any further endovascular treatment or surgery.
Infective pathology
Infection in the MS most often arises from odontogenic infection or following dental manipulation. Other uncommon causes are extension from parotid infection, malignant otitis externa or tonsillar abscess.
Clinical presentation
Infection in MS is most often seen in the elderly population and in those with compromised dental hygiene. The typical clinical presentation is with trismus, facial swelling, pain and fever.
Imaging findings
The infective pathology of MS progresses from oedema to phlegmon to abscess formation. Phlegmon in MS is infectious tissue without necrosis, while abscess has drainable infected debris within. Osteomyelitis may be seen both as a precursor of or sequelae to infection of the masticator space.
• CT: Phlegmon is seen as heterogeneously enhanced muscles without rim enhancement on CECT (Fig. 3.17.1.5A–C). Frank abscess is seen as a peripherally enhancing collection in the MS (Fig. 3.17.1.5B). Underlying mandibular ramus and posterior body may show features of osteomyelitis with cortical destruction and periosteal elevation. Chronic osteomyelitis is seen as cortical thickening, periosteal reaction and sequestrum formation. Sinus tract if any is seen as a curvilinear tract extending from the mandible to the abscess on CECT.
• MRI: In a phlegmon, the involved muscles are bulky and appear iso to hypointense on T1 weighted MR, hyperintense on T2 weighted MR images with homogenous enhancement following gadolinium injection. Rim enhancing fluid collection involving the muscles of mastication indicate abscess formation. There may be accompanying stranding in overlying subcutaneous fat suggesting cellulitis. Osteomyelitis may be seen as loss of cortical signal void and normal bright signal of marrow on T1W images. T2 and STIR images depict oedema within the marrow and show subperiosteal fluid if any. Sinus tract is better visualized on enhanced MRI than on CT.
Fig. 3.17.1.5Masticator space abscess. Contrast-enhanced axial (A) and coronal (B) CT images at soft-tissue algorithm show bulky ill-defined muscles involving masticator space ( white arrow) with overlying cellulitis seen as fat stranding. Well-defined pockets of fluid attenuation with air foci suggestive of abscesses are also seen in parapharyngeal space ( black arrow) and submandibular space ( curved white arrow). There is overlying skin ulceration ( white arrow head) and extension to suprazygomatic portion ( star) of MS. Axial bone window (C) shows a missing tooth ( black arrow with white outline), the likely cause of infection. Communication between PPS and posterior portion of submandibular space explains the spread from parapharyngeal space to submandibular space.
Cellulitis/phlegmon of MS needs to be differentiated from a frank abscess as the patient management is different in both cases. More aggressive treatment is required in case of an abscess formation.
The infectious process may extend to involve the adjacent parapharyngeal, retropharyngeal and parotid spaces. It may extend to the skull base as the superior extent of MS reaches the skull base. Internal carotid artery spasm may occur if infection involves the parapharyngeal or retropharyngeal space.
Uncommon infection/inflammation
Uncommon infections involving the MS include fungal pathogens (aspergillus, mucor), tuberculous infections and actinomycosis. The imaging findings are not definitive and may simulate a neoplastic process. Parasitic infections such as hydatid cyst and cysticercus may also involve the muscles of mastication. Hydatid cyst is seen as a unilocular or multilocular cyst with internal daughter cyst formation. Cysticercus involving the muscles of mastication is seen as a small rim enhancing lesion and may show the characteristic mural nodule (Fig. 3.17.1.6).
Fig. 3.17.1.6Myocysticercus of masseter muscle. In a known patient of neurocysticercosis on brain MRI, axial postgadolinium MR image shows a round rim-enhancing lesion ( white arrow) with a small mural nodule ( black arrow with white outline) within the right masseter muscle.
Granulomatosis with polyangiitis (previously called Wegener granulomatosis) can rarely involve MS either by direct spread or along the V3 nerve. This disease is characterized by a triad of necrotizing granuloma in the respiratory tract, necrotizing vasculitis and glomerulonephritis. It manifests as extensive inflammatory changes in masticator space and buccal space. Inflammatory changes involve muscles of mastication and extend superiorly to skull base, with associated thickening and enhancement of third division of trigeminal nerve.
Differential diagnosis
• Osteonecrosis of mandible can be hard to differentiate from osteomyelitis of mandible. The clinical history of prior radiation/antiangiogenic medication is a clue to the correct diagnosis. Soft-tissue collections are more frequently seen with osteomyelitis than osteonecrosis.
• Malignant pathology of MS lacks the cellulitis or myositis that often accompanies infection. Clinical features need to be kept in mind to make the distinction. Advanced imaging techniques such as MR diffusion and MR spectroscopy are the other emerging investigational tools in differentiating between inflammatory and malignant masses of MS. Restricted diffusion is seen in malignancy and abscess, while inflammatory pathology usually depicts facilitated diffusion. MR spectroscopy reveals high choline/creatine ratio in malignancy in contrast to an inflammatory process. In cases where the distinction is not possible, imaging provides an accurate map to guide biopsy.
MS INFECTION – PEARLS AND PITFALLS
• MS infection is more common than MS tumours.
• The imaging appearance of infections and sarcomas in MS can overlap as cortical destruction, periosteal reaction and accompanying soft tissue may be seen in both. Clinical information is paramount in making the distinction.
• In patients with masticator space abscess, the images must be carefully assessed for odontogenic source of infection, presence of osteomyelitis and accurate extent of the abscess for guiding further management.
Benign tumours
Nerve origin
Neurogenic tumour in MS is most commonly a schwannoma, arising from the mandibular division of trigeminal nerve (V3). Neurofibroma (NF) is an uncommon neurogenic tumour to involve the V3 and is usually seen as part of NF1.
Schwannoma
Schwannoma originates from the Schwann cells (peripheral nerve sheath) of V3 and displaces V3 nerve fascicles without infiltration.
Clinical features.
Schwannoma of MS most commonly presents in third to fourth decades of life. Patients with NF2 may present with schwannomas at an earlier age. Most often, schwannoma presents as an asymptomatic mass. They can present as an asymptomatic mass; however, facial numbness, facial pain and difficulty in chewing (weakness of muscles of mastication) may be the presenting complaints.
Imaging findings.
MS schwannoma is a well-defined ovoid to fusiform mass seen along V3 branch of trigeminal nerve.
• CT: Schwannoma is mildly hyperdense to muscle and shows mild to moderate enhancement following contrast administration. On dynamic scan, delayed images at 2–3 min may show marked enhancement owing to poor venous drainage in a schwannoma. Homogeneous enhancement is seen in small lesions, while larger lesions may show heterogeneous enhancement owing to the presence of internal cystic change or haemorrhage.
Smooth enlargement of involved foramen is noted, most notably the foramen ovale. Mandibular foramen, inferior alveolar canal and mental foramen can also enlarge in the rare case of a schwannoma affecting the distal nerve.
Secondary to V3 involvement, denervation atrophy of ipsilateral muscles of mastication may occur, resulting in enlarged enhancing muscles in the acute stage and atrophic fatty muscles in the chronic stage. Care must be taken not to mistake the ipsilateral affected bulky side for a mass lesion in the acute stage and normal muscles of mastication on the contralateral side as a mass lesion in the chronic stage.
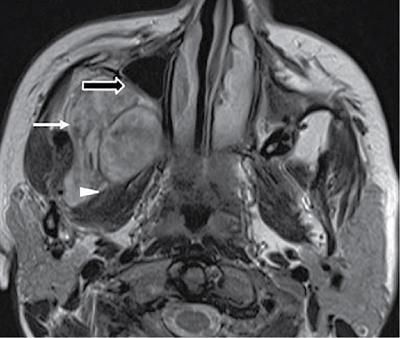
• MRI is the imaging modality of choice. The mass appears of intermediate signal on T1-weighted MR images and hyperintense on T2-weighted MR images. A target pattern on T2-weighted MR images with decreased central signal, characteristically described for NF, may also be seen in schwannomas (Fig. 3.17.1.7). Internal haemorrhage may result in hypointense signal on T2-weighted sequence.
Fig. 3.17.1.7Masticator space nerve sheath tumour. T2W axial MR shows a well-defined mass ( white arrow) in right masticator space, deviating the medial pterygoid muscle medially ( arrowhead) and remodelling the posterior wall of the maxillary antrum ( black arrow with white outline). The lesion appears hyperintense on T2W sequence with few hypointense areas within.
Differential diagnosis
• NF of V3 is less common than a V3 schwannoma. It is mostly seen in association with NF-1. Plexiform NF is a common form of NF to affect the cranial nerves.
• Venous vascular malformation (VVM) is a common lesion in MS and may mimic a neurogenic tumour. However, VVM is not centred over V3, and there is no accompanying foraminal enlargement. It is usually a multilocular mass with heterogeneous enhancement. On dynamic scan, it shows delayed patchy enhancement following gadolinium injection. Phleboliths when seen are characteristic of venous malformations.
• In the presence of a known primary head and neck malignancy, perineural spread along V3 may be considered. Perineural spread can result in involvement of the entire neural pathway, and enhancement of the nerve precedes nerve enlargement unlike the mass that is more often seen in schwannoma.
• MS sarcoma is not centred over V3 nerve and is a more aggressive mass with accompanying bone destruction/periosteal reaction.
Neurofibroma
NF is an uncommon neurogenic tumour to involve V3 nerve. It is mostly seen in association with NF1. A target pattern has been described on T2-weighted MR images for NF where there is decreased central signal and increased peripheral signal owing to a fibrous core. However, this is not exclusive to NF and can be seen in schwannoma as well. Plexiform NF extends longitudinally along the branches of trigeminal nerve and is diagnostic of NF1. The involvement of multiple fascicles of the nerve gives a network-like appearance to the tumour. Central hypointensity on T2-weighted MR image giving the target appearance may be seen in various involved nerve fascicles. Plexiform NF carries a high risk of malignant transformation to malignant peripheral nerve sheath tumour (MPNST).
NEUROGENIC TUMOURS IN MS – PEARLS AND PITFALLS
• Neurogenic tumour must be considered when a mass lesion is centred over V3 nerve and shows intracranial extension with waist formation at foramen ovale.
• Schwannoma of V3 is commoner than a neurofibroma.
• When a schwannoma of V3 is detected, the stigmata of NF2 must be looked for.
• Neurofibroma is commonly seen in association with NF1.
• In a known case of primary head and neck malignancy, perineural spread of malignancy affecting the V3 nerve is much more likely rather than a primary neurogenic tumour.
Bony origin
Cysts and tumours of the jaw form a large spectrum of MS pathology. However, these are discussed elsewhere in the book, in the chapter on “Imaging of the Jaws”.
Malignant tumours of masticator space
Malignant tumours of the MS include intrinsic tumours (sarcomas, non-Hodgkin’s lymphoma [NHL]) as well as extrinsic masses which may invade the masticator space (squamous cell carcinoma of the oral cavity and nasopharynx, sinus malignancy, parotid malignancy and perineural spread along V3 nerve).
Sarcomas
These include a variety of tumours including osteosarcoma, chondrosarcoma, rhabdomyosarcoma, Ewing’s sarcoma, synovial sarcoma, leiomyosarcoma, liposarcoma, primitive neuroectodermal tumours (PNETs) and MPNSTs. The imaging features of the relatively common masses are described in the following.
Osteosarcoma
Osteosarcoma is the most common sarcoma of the masticator space. It usually arises from bone, i.e. the mandible, but can also arise less commonly from extraosseous soft tissues.
Clinical presentation.
Unlike the long bone osteosarcoma where it is usually seen in childhood, patients with mandibular osteosarcoma present in the third and fourth decades of their life with a male predilection. Paget’s disease, fibrous dysplasia and previous irradiation to craniofacial region are predisposing factors for secondary osteosarcomas. Patients present with swelling of jaw, sometimes accompanied by numbness of the affected region and limited jaw motion.
Imaging.
The most common site affected is the body of mandible followed by angle, symphysis and ramus.
• Radiograph (orthopantomogram): Osteosarcoma should be suspected on a radiograph when there is a focal, destructive, poorly marginated lesion with osteolytic to mixed to osteosclerotic pattern of bone involvement. Sunray appearance of periosteal reaction may also be seen.
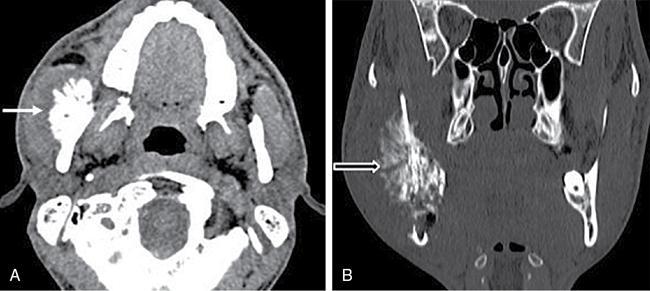
• CT: Similar to the radiograph, CT shows an ill-defined lesion with lytic/mixed/sclerotic type of bone destruction, osteoid pattern of matrix mineralization resulting in “cumulus cloud” appearance (Fig. 3.17.1.8A). Internal matrix as well as extension into adjacent soft tissues is better depicted on CT than on a radiograph. “Sunray appearance” or “hair-on-end appearance” (Fig. 3.17.1.8B) are terms used to describe the extensive and aggressive periosteal reaction associated with osteosarcoma. However, this appearance is not specific for osteosarcoma.
• MRI: Osteosarcoma is of low-to-intermediate signal intensity on T1-weighted images and shows high signal intensity on T2-weighted images. Areas of signal void representing new bone formation and calcifications are also seen within the lesion. There is heterogeneous enhancement of the soft-tissue component following gadolinium injection.
Fig. 3.17.1.8Osteosarcoma of mandibular ramus. Axial soft tissue (A) and coronal bone (B) algorithm CT images show an ill-defined lytic lesion in ramus of right mandible with an aggressive sun burst type of periosteal reaction ( black arrow with white outline) and accompanying heterogenous soft tissue ( white arrow).
Differential diagnosis
• Infection MS is the most frequent cause of mass in MS. Clinical features of sepsis point to the diagnosis of infection. Rim-enhancing fluid collection favours an abscess. Bony sequestrum formation may be seen.
• Chondrosarcoma is rare in the head and neck regions; it tends to occur around the temporomandibular joint and is less aggressive compared with osteosarcoma. “Ring and arc” pattern of calcification in the mass is highly characteristic of chondrosarcoma. However, it can be sometimes difficult to differentiate between the two entities on imaging alone.
• Ewing sarcoma is also a rare sarcoma in the head and neck regions presenting at a relatively younger age. Expansile lytic lesion and “onion-skin” type of periosteal reaction are the typical imaging findings.
• Fibrous dysplasia presents in adolescents and young adults. On imaging, fibrous dysplasia shows “ground-glass appearance” and aggressive periosteal reaction is not seen.
• Metastases commonly involve the posterior body and angle of mandible. On imaging, they can be lytic or sclerotic depending on the primary tumour and may show extension into adjacent soft tissues along with aggressive periosteal reaction. Common primary tumour sites include lung, breast, kidney, prostate and thyroid.
Chondrosarcoma
It is a rare malignant tumour of the craniofacial region, characterized by cartilaginous matrix. Primary chondrosarcoma arises de novo, whereas secondary chondrosarcoma arises from preexisting conditions such as osteochondroma, enchondroma, Paget’s disease or radiation induced injury. They are found predominantly in symphysis, coronoid and condyloid process of the mandible as these parts of the mandible undergo enchondral ossification.
Clinical presentation.
Patients usually present in their fourth to fifth decades of life. The common clinical presentation is painless jaw swelling; however, there may be headache, paresthesia and loosening of teeth with premature exfoliation.
Imaging
• Radiograph (panoramic orthopantomogram): The tumour presents as a unilocular or multilocular area(s) of intramedullary radiolucency with irregular margins. Focal calcification may be seen in 45%–80% of cases. Widening of periodontal ligament space is considered an early sign of chondrosarcoma.
• CT: Chondrosarcoma is seen as a soft-tissue mass with multiple foci of calcifications, adjacent areas of bone erosion, destruction of overlying cortex and/or endosteal scalloping. Calcification is dependent on the grade of the tumour. While ring and arc pattern of calcification is seen in low-grade tumours, amorphous calcification is characteristic of high-grade tumours. Slow-growing tumours may cause reactive cortical thickening instead of cortical erosion. There is no/or mild periosteal reaction. Heterogeneous enhancement is seen on postcontrast scan, which may be predominantly peripheral.
• MRI: The tumour appears hypointense on T1-weighted images relative to the bone matrix. Owing to chondroid matrix, it typically appears hyperintense on T2-weighted images. Areas of signal void and heterogeneity on all sequences represent calcification within. On postgadolinium imaging, the soft-tissue mass may show focal or diffuse enhancement.
Differential diagnosis
• Infection – If chondrosarcoma has no calcification within, it may mimic MS infection. Rim-enhancing fluid collection in the clinical setting of sepsis suggests abscess. Bony sequestrum formation may be seen.
• Osteosarcoma – Osteosarcoma of the jaw presents at a relatively earlier age and tends to be more aggressive with respect to bone destruction and periosteal reaction.
• Epithelial odontogenic tumour, ossifying fibroma and cavernous haemangioma of bone can sometimes be confused with a chondrosarcoma owing to internal calcific foci; however, these are benign masses. Presence of a large aggressive soft-tissue mass with erosion of adjacent bone in the appropriate age group favours the diagnosis of chondrosarcoma.
Rhabdomyosarcoma
A variety of soft-tissue sarcomas tend to occur in the masticator space, the most common being rhabdomyosarcoma especially in the paediatric age group. It takes origin from differentiated mesenchymal cells.
Clinical presentation.
The mean age of presentation is between 5 and 6 years, and nearly 72%–81% of patients are younger than 10 years of age. Slight male preponderance is reported. The clinical signs and symptoms include pain, restricted jaw movement, facial deformity and loss of sensation in the affected region. The lesion on local examination may demonstrate smooth or grape-like lobulated surface with fixation to surrounding tissues.
Imaging
• Radiograph: It is of extremely limited value. The tumour is seen as a relatively well-defined soft-tissue mass with associated lytic bone destruction.
• USG: The role of ultrasound is limited due to its inability in evaluating deep extension of tumour. Its main role is to safely guide a needle biopsy of the primary tumour and assess any regional nodal disease.
• CT: A relatively well-circumscribed mass is seen with associated lytic destruction of bone. Due to ionizing radiation, CT is not the investigation of choice in children. It is mainly used to identify any lung metastases.
• MRI: Most of the rhabdomyosarcomas are hypointense on T1-weighted images with a variable appearance on T2-weighted images owing to differences in internal cellularity, necrosis and haemorrhage. Highly cellular variety of rhabdomyosarcoma may appear hypointense on T2-weighted images. Most tumours show moderate homogeneous contrast enhancement following gadolinium injection.
Differential diagnosis
• Ewing sarcoma is a common bone tumour in children but is uncommon in the MS. Expansile lytic lesion and “onion-skin” type of periosteal reaction are the typical imaging findings.
• NHL-associated nodal disease, involvement of Waldeyer’s ring and other extranodal and extralymphatic sites (paranasal sinuses, orbits) suggest the diagnosis of lymphoma.
• Vascular anomalies include haemangioma and vascular malformation. Haemangioma is the most common benign tumour of masticator space in children and does not show any infiltration or bone destruction. Lymphatic malformations are multiloculated cystic lesions which show low signal on T1W and high signal on T2 W images. A multilobulated progressively enhancing mass with phleboliths within is highly characteristic of a venous malformation.
SARCOMA IN MS – PEARLS AND PITFALLS
• When there is no history of sepsis or known squamous cell carcinoma of head and neck region, a mass in masticator space is most likely a sarcoma; particularly in children.
• Osteosarcoma is the most common sarcoma of the masticator space.
• MRI is the best modality to study the extent of bone marrow involvement seen as replacement of normal T1 hyperintense fatty bone marrow by hypointense tumour. Superior soft-tissue resolution allows better assessment of the extent. CT depicts subtle bone changes and calcification pattern.
• “Cumulus cloud” pattern of new bone formation and “sunburst periosteal reaction” are pointers to the diagnosis of osteosarcoma.
• “Ring and arc” or amorphous calcification when present is characteristic of chondrosarcoma.
• Rhabdomyosarcoma is the most common sarcoma of masticator space in the paediatric age group.
• Irrespective of appearances of sarcomas, biopsy is needed for precise diagnosis and management.
Non-Hodgkin’s lymphoma
NHL is malignant proliferation of the lymphoid tissue, which also affects extranodal sites such as the gastrointestinal tract and the head and neck regions. Masticator space is an uncommon site for extranodal NHL in the craniofacial region. NHL can rarely involve the jaw (discussed in chapter on “Imaging of the Jaw”), and primary involvement of muscles of mastication is rarer. It may often not be possible to predict whether the NHL began in the bone or the muscles.
The patients usually present in the fifth and sixth decades of their life, mean age of presentation being 62.5 years, with a slight male preponderance.
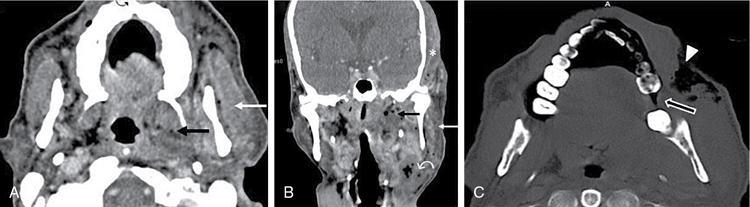
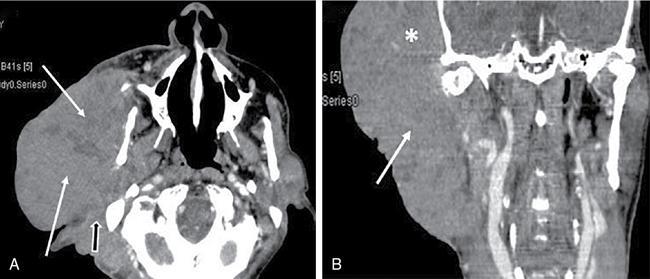
On CT, it is seen as an ill-defined isodense to hypodense mass, infiltrating the muscles of mastication (Fig. 3.17.1.9A–B). Postcontrast images show heterogeneous contrast enhancement. Bone destruction may be seen. On MRI, the imaging findings are nonspecific; however, lymphoma usually appears as low intensity mass on T2-weighted images. On diffusion-weighted MR images, lymphoma shows diffusion restriction owing to high cellularity. Perineural spread can also occur with lymphoma. Small round cell tumours, including sarcomas, mimic NHL on imaging. An aggressive mass lesion in MS along with involvement of extranodal sites and cervical nodes is a strong pointer towards the diagnosis of lymphoma.
Fig. 3.17.1.9Masticator space lymphoma. CECT axial (A) and coronal (B) show a bulky relatively homogeneously enhancing mass ( arrow) involving masseter and temporalis muscle ( star). The mass extends to sternocleidomastoid muscle ( black arrow with white outline) and posterior cervical space. Underlying bones were normal.
Extrinsic
Perineural spread along mandibular nerve (V3)
Head and neck malignancies commonly spread along the cranial nerves and/or their branches to distant sites away from the primary tumour. Perineural spread (PNS) can be defined as dissemination of tumour from its primary location along the nerve pathway, using the nerve as a scaffold. It needs to be emphasized that perineural invasion is a separate entity from perineural spread. Perineural invasion refers to histological finding of tumour cell infiltration of a nerve, while perineural tumour spread is macroscopic nerve involvement, which is radiologically and clinically evident. The most common histologic types of tumours that spread along the neural pathways include squamous cell carcinoma, adenoid cystic carcinoma, high-grade mucoepidermoid carcinoma, desmoplastic variant of melanoma and advanced cases of NHL.
The nerve(s) primarily involved in perineural spread of tumour to masticator space is the mandibular nerve (V3) and its branches. The two most common branches of mandibular nerve that are involved in neoplastic perineural spread are the auriculotemporal nerve and the inferior alveolar nerve.
• Auriculotemporal nerve branches from the mandibular nerve just below the foramen ovale. Few of its branches innervate the lateral and superior aspect of face. The parasympathetic fibres of auriculotemporal nerve anastomose with facial nerve branches in the substance of the parotid gland. This results in spread of malignant neoplasms of parotid gland as well as tumours from the lateral facial region to the masticator space via the perineural pathway.
• Inferior alveolar nerve courses through the mandible after entering it through the mandibular foramen along the medial aspect of mandibular ramus and exits as mental nerve from the mental foramen on the anterior surface of the body of mandible. During its course, it innervates the chin, lower lip, mandibular teeth and gingival mucosa, and therefore the malignancies from these regions can reach the masticator space by tracking along the nerve.
Clinical presentation.
PNS may be asymptomatic or may present with pain, paraesthesia, numbness and motor weakness. When mandibular (V3) division of trigeminal nerve is involved, the weakness involves muscles of mastication, anterior belly of digastric, mylohyoid and tensor veli palatini muscle.
Imaging.
Perineural spread mostly progresses from the nerve branches centripetally towards the brain. When the tumour reaches sites of interneuronal communication, e.g. the pterygopalatine fossa, PNS may be seen to occur centrifugally exiting the skull again along a different nerve. MRI is the imaging modality of choice for evaluating perineural spread of tumour, owing to its superior soft-tissue contrast and less artefacts compared with CT. Postcontrast T1-weighted high spatial resolution volumetric sequence with fat saturation is considered the most sensitive sequence to assess perineural spread. The fat saturation allows the enhancing tumour to be easily delineated from fat-rich spaces such as orbits, pterygopalatine fissure and neurovascular foramina. Precontrast non–fat-saturated T1 sequence is another helpful sequence that enables visualization of obliteration of neural foraminal fat by the tumour mass.
Imaging features of perineural tumoural spread can be broadly categorized as direct and indirect.
Direct signs
CT: CT scan show enhancement of the nerves and widening of affected neural foramina and bone erosion with partial or complete effacement of perineural fat (Fig. 3.17.1.10C). It is important to also evaluate the bone window algorithm images carefully.
MRI: Diffuse enhancement, thickening and nodularity of involved nerve(s) with obliteration of adjacent perineural fat and widening of neural foramina with or without bone erosion are the direct signs of PNS. Other signs include asymmetric bulging of the cavernous sinus and loss of CSF signal in the Meckel’s cave (Fig. 3.17.1.10A). Skip lesions may also be seen on imaging.
Fig. 3.17.1.10Nasopharyngeal carcinoma with perineural spread to masticator space. Contrast-enhanced coronal (A) MRI shows an enhancing mass in the left nasopharynx ( white star) extending through a widened left foramen ovale ( black star) into the left cavernous sinus ( white arrow head), which appears bulky with a convex lateral margin. There is accompanying atrophy of left masseter muscle ( black arrow with white outline in B) with fatty changes indicating chronic denervation atrophy and bulky neck lymph nodes ( white arrows in B).Coronal CT (C) of same patient shows the widened left foramen ovale ( black star).
Indirect signs.
Indirect signs are due to denervation atrophy of muscles secondary to PNS.
CT: Muscle oedema is seen in the acute stage, while reduced bulk of muscles and eventual fatty atrophy is seen in the chronic stage.
MRI: In acute to subacute stage, the affected muscles appear T2 hyperintense and show increased enhancement on postgadolinium scans. In chronic stages, there is atrophy with fatty replacement (Fig. 3.17.1.10B).
Differential diagnosis
• Nerve sheath tumours – Tumours such as schwannoma and NF also present with enlargement of nerves, which show enhancement following contrast injection. Perineural spread, however, may result in involvement of the entire neural pathway, and enhancement of the nerve precedes nerve enlargement.
• Invasive fungal infection – Aspergillosis and mucormycosis are the two most common fungal infections which present with thickening and enhancement of nerves mimicking tumours with perineural spread. However, they usually affect immunocompromised patients.
• Meningeal disorders – Meningeal inflammatory conditions such as sarcoidosis, syphilis or Lyme disease and meningeal carcinomatosis can also exhibit nerve enlargement and enhancement closely mimicking perineural spread of tumour.
Only gold members can continue reading. Log In or Register to continue