Fig. 3.1
Congenital CMV infection in a neonate with anemia, sensorineural hearing loss, and seizures. (a) US of brain shows dilation of both lateral ventricles with abnormal echogenic lining of the ventricular walls (arrows) suggesting calcifications. (b) Multiple linear echogenicities in both thalami (arrow) are seen as lenticulostriate vasculopathies. (c) T1-weighted image shows dilated ventricles with high-signal intensities along the ventricular walls. Wide subarachnoid spaces suggest diffuse brain atrophy. (d) T2-weighted image shows low signal intensities lining the lateral ventricles (arrows) suggesting the ventricular wall calcifications. Widening of the retrocerebellar subarachnoid space is seen
3.4.2 Congenital Toxoplasmosis
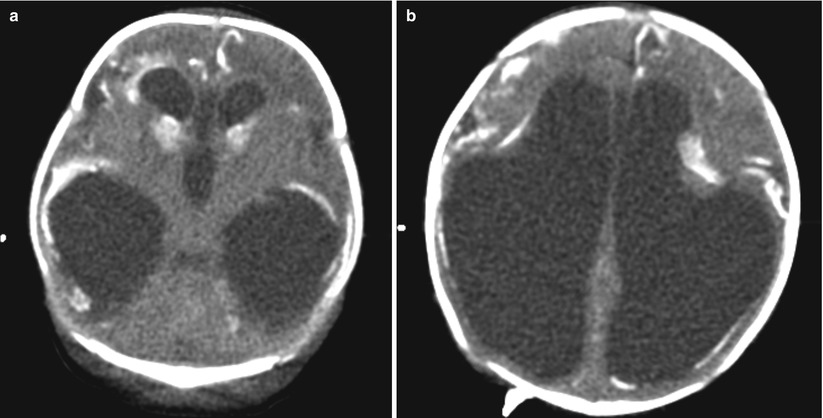
Fig. 3.2
A neonate with congenital toxoplasmosis. (a) CT shows markedly dilated lateral and third ventricles with ventricular wall calcifications. (b) Severe cortical thinning with multiple parenchymal and deep nuclear calcifications along with the ventricular wall calcifications
3.4.3 Hemophilus Meningitis
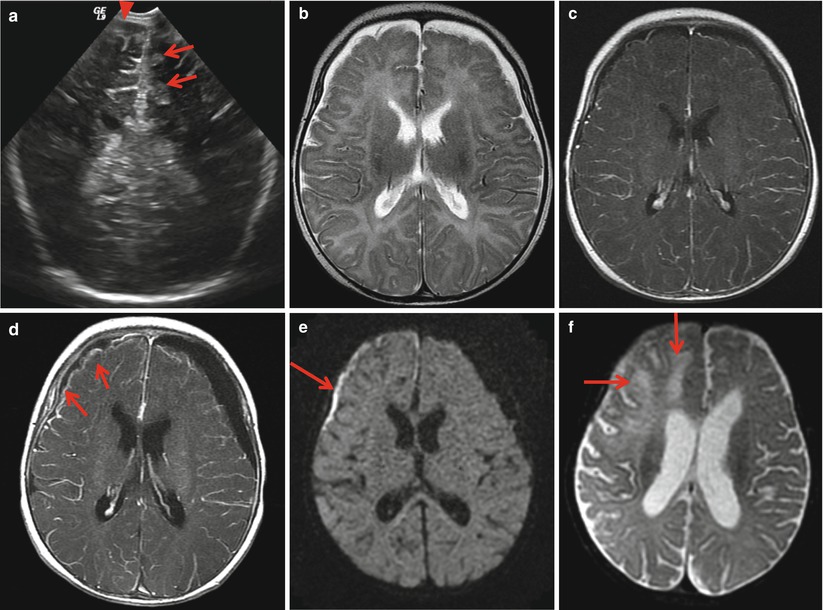
Fig. 3.3
A 3-month-old infant with hemophilus meningitis. (a) US shows increased echogenicities of the cerebral sulci (arrows) and extra-axial fluid collection in the frontal region (arrowhead). (b) T2-weighted image shows extra-axial fluid collections along both frontal region. (c) Postcontrast image shows no remarkable meningeal enhancement. (d) Follow-up image after 1week shows progression of hydrocephalus and extra-axial fluid collections. Meningeal enhancement is more prominent along the right-side fluid collection (arrows). (e) Diffusion image suggests complicated fluid collection in the right frontal region (arrow), such as subdural empyema. (f) Another week’s follow-up shows parenchymal edema in the right frontotemporal lobe (arrows), suspecting complicated infarction and progression of ventriculomegaly
3.4.4 Streptococcal Meningitis
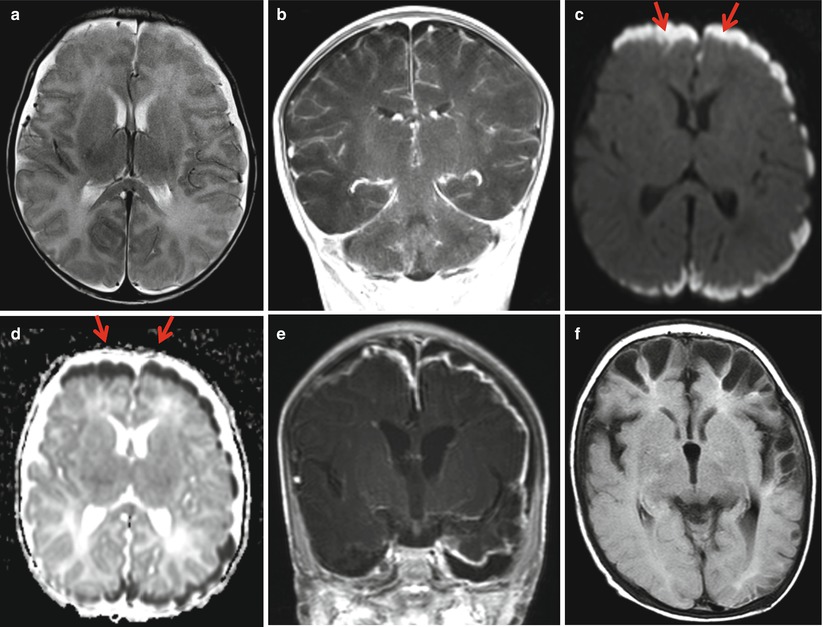
Fig. 3.4
A neonate with streptococcal meningitis. (a) T2-weighted image shows small amount of extra-axial fluid collections along the frontotemporal region. (b) Postcontrast MR image shows subtle meningeal enhancement over the convexity. (c) Diffusion and (d) ADC images show restricted diffusion of the extra-axial fluid (arrows), suspecting a complication of subdural empyema. (e) Two-week follow-up image shows strong enhancement of the meninges under the fluid collections. Ventricles are moderately dilated. (f) 2-month follow-up study shows multifocal cystic encephalomalacia along the frontotemporal cortex due to gyral infarctions complicated by bacterial meningitis
3.4.5 Tuberculous Infection
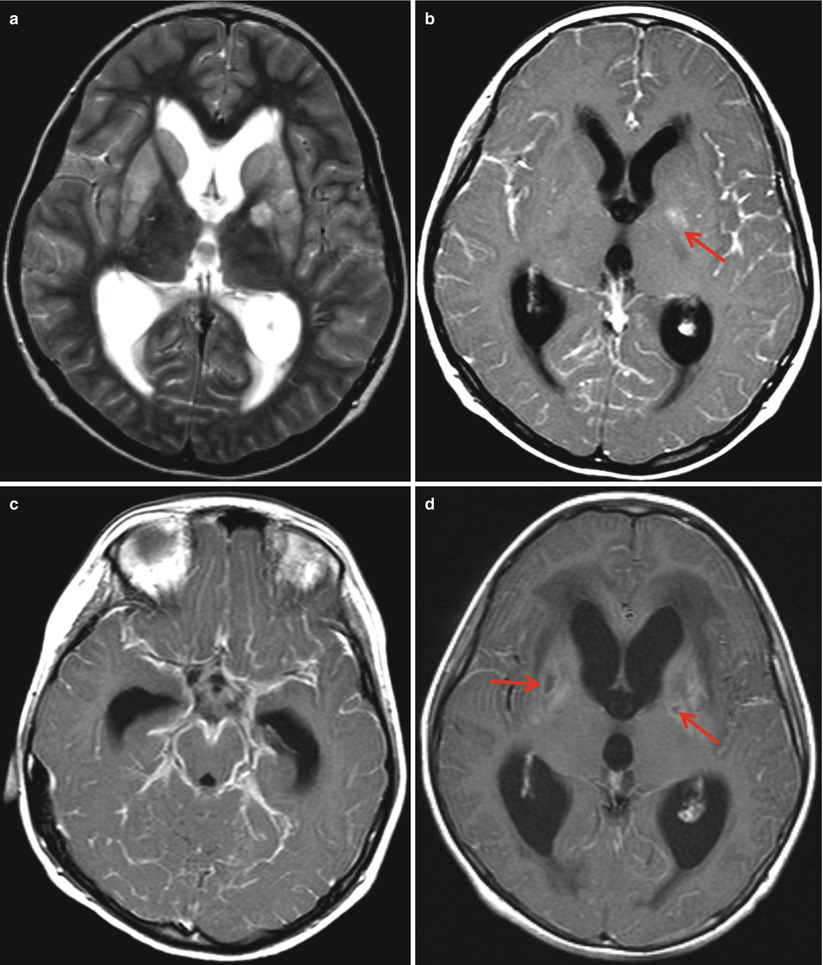
Fig. 3.5
Tuberculous meningitis in an 11-month-old boy. (a) T2-weighted image shows moderate hydrocephalus with bilateral basal ganglia edema. (b) Postcontrast image shows diffuse leptomeningeal enhancement and focal nodular enhancements in the left globus pallidus (arrow). (c) The meningeal enhancements are more extensive in the basal cistern than the cortical surface. (d) T1-weighted image after 1 month shows progression of hydrocephalus and periventricular edema. Focal low signals of both lentiform nucleus (arrows) suspecting focal encephalomalacia
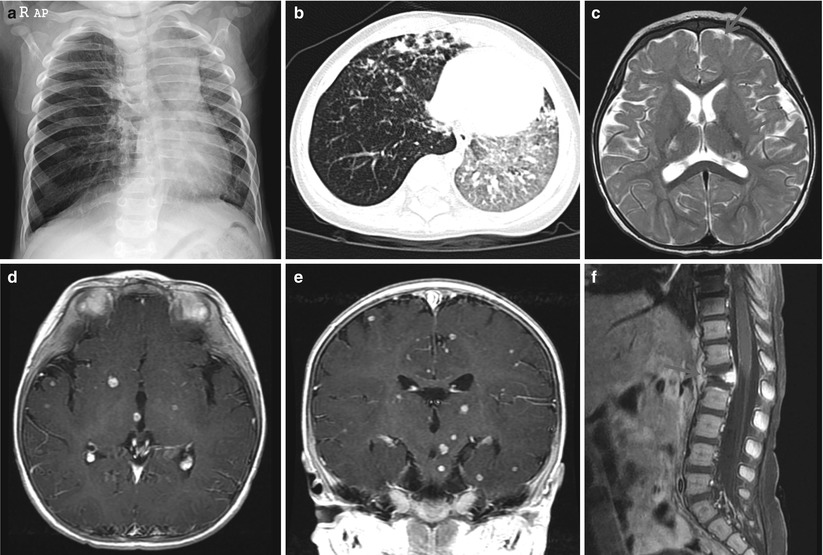
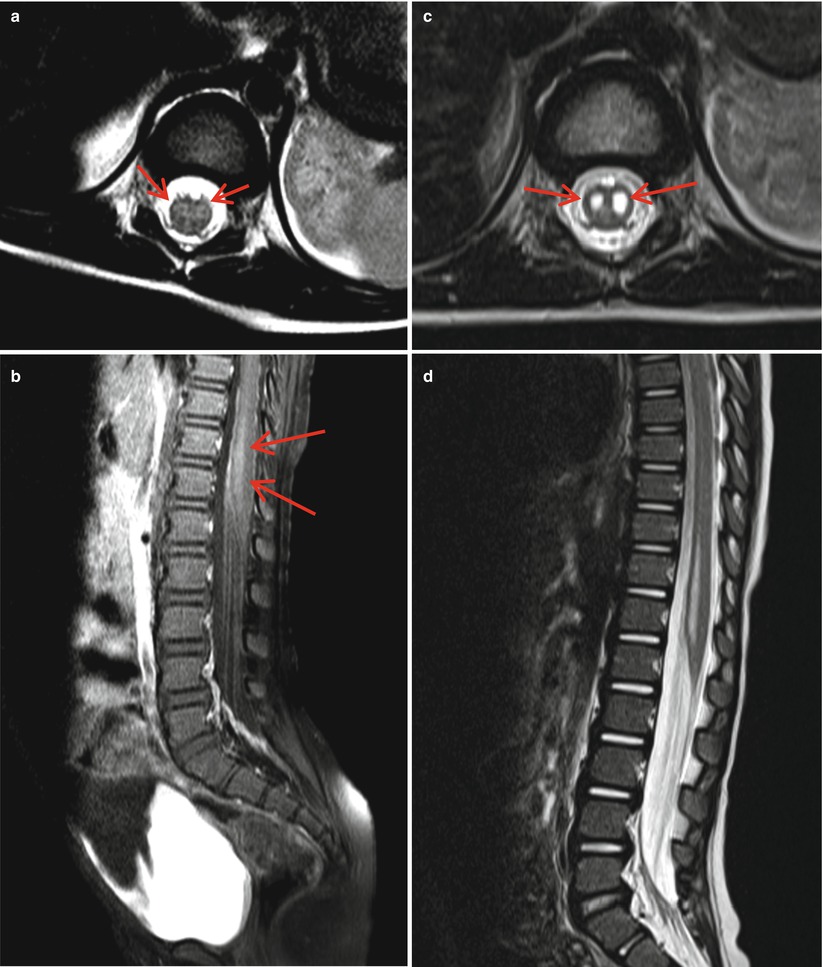
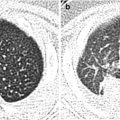
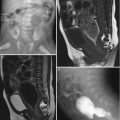
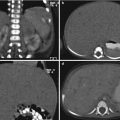
Fig. 3.6
Disseminated tuberculomas are in the brain and spine of a 9-month-old boy. (a) Plain chest radiograph shows decreased left lung volume with subtle fine nodules in the left lung. Right lung shows hyperaeration and focal atelectasis in the suprahilar area. (b) Miliary nodules and bronchopneumonic infiltrations are well demonstrated with CT. The left lung is hyperaerated. (c) T2-weighted image shows multiple nodules in the deep nuclei. Right posterior thalamic lesion shows a nodule with central low signal. (d, e) Multiple ring-enhancing nodules are disseminated in the cerebrum, brainstem, and cerebellum (not shown). (f) Tuberculous spondylitis shows collapse of the L1 body and pre- and post-vertebral enhancing lesion (arrow)
3.4.6 Candidiasis
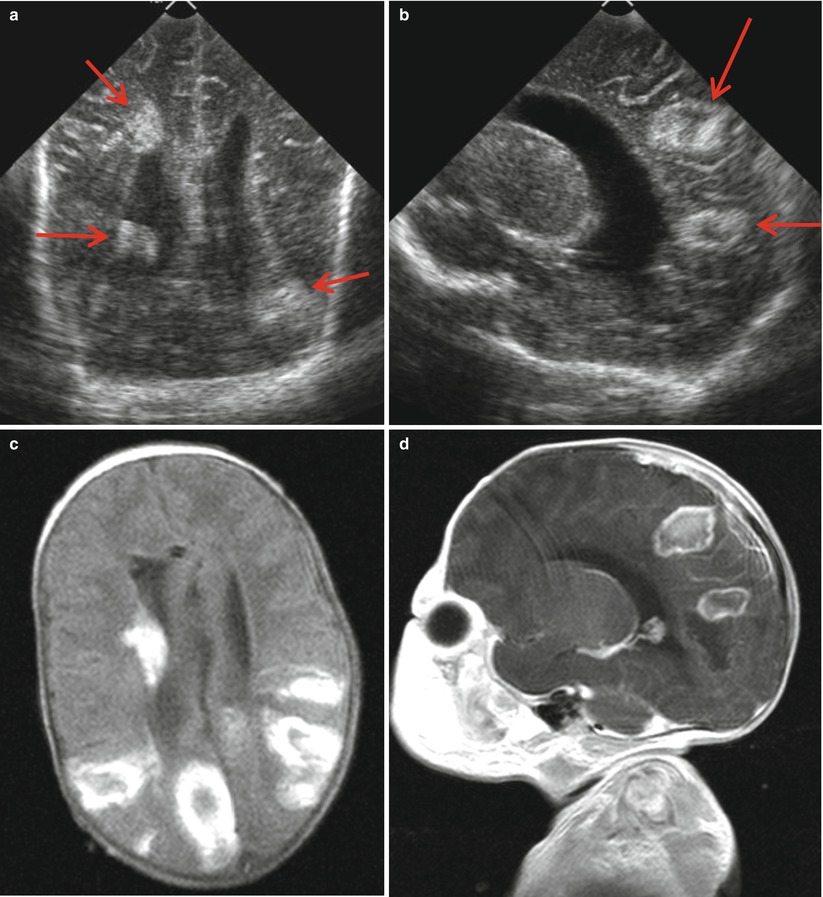
Fig. 3.7
A 6-week-old baby with myelomeningocele. (a, b) US shows hydrocephalus and multiple cavitary echogenic mass lesions in the cortical and periventricular area proven to be candidiasis (arrows). (c) T1-weighted image shows multiple hemorrhagic lesions suggesting hemorrhagic infarction. (d) Postcontrast image suggests abscess formation due to septic embolism
3.4.7 Herpes Simplex Encephalitis
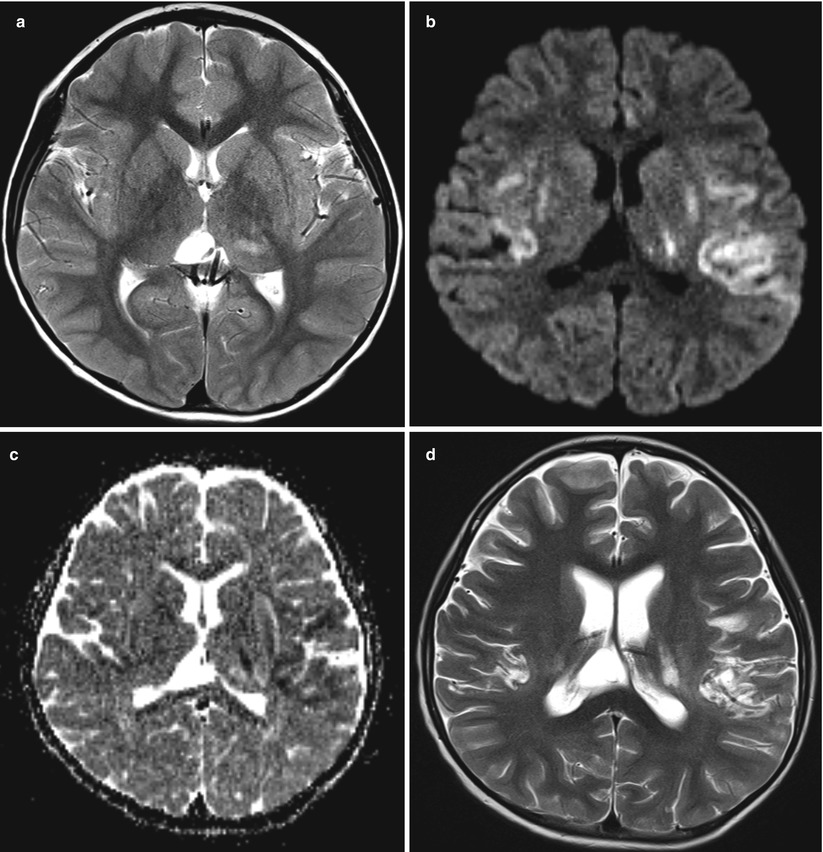
Fig. 3.8
A 5-year-old boy with herpes simplex encephalitis. (a) T2-weighted image shows subtle swelling of the temporal lobe and thalamus and posterior cingulate gyrus, predominantly in the left side. (b) Diffusion and ADC (c) images after 3 days show restricted diffusion in both temporal and left thalamus. (d) Two-week follow-up image reveals rapid parenchymal loss of the involved area with mild brain atrophy
3.4.8 Varicella Encephalitis
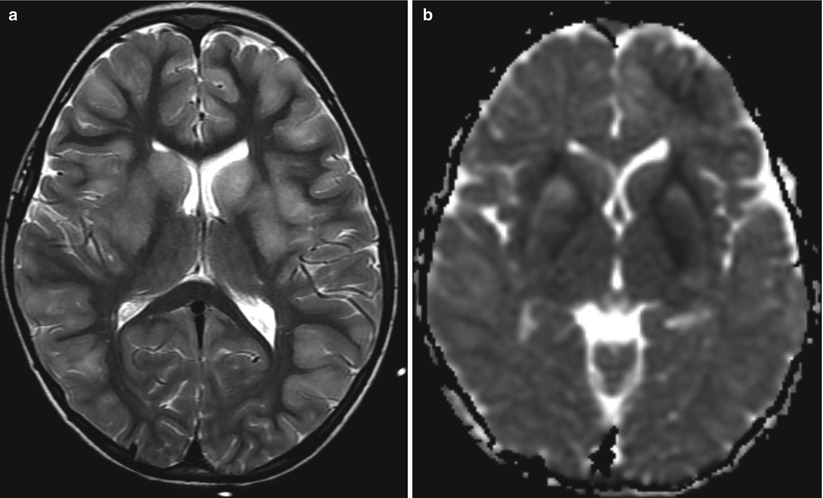
Fig. 3.9
Varicella encephalitis. (a) T2-weighted image shows disseminated lesions in the cortex and the basal ganglia. (b) Diffusion image shows restricted diffusion of the lesions
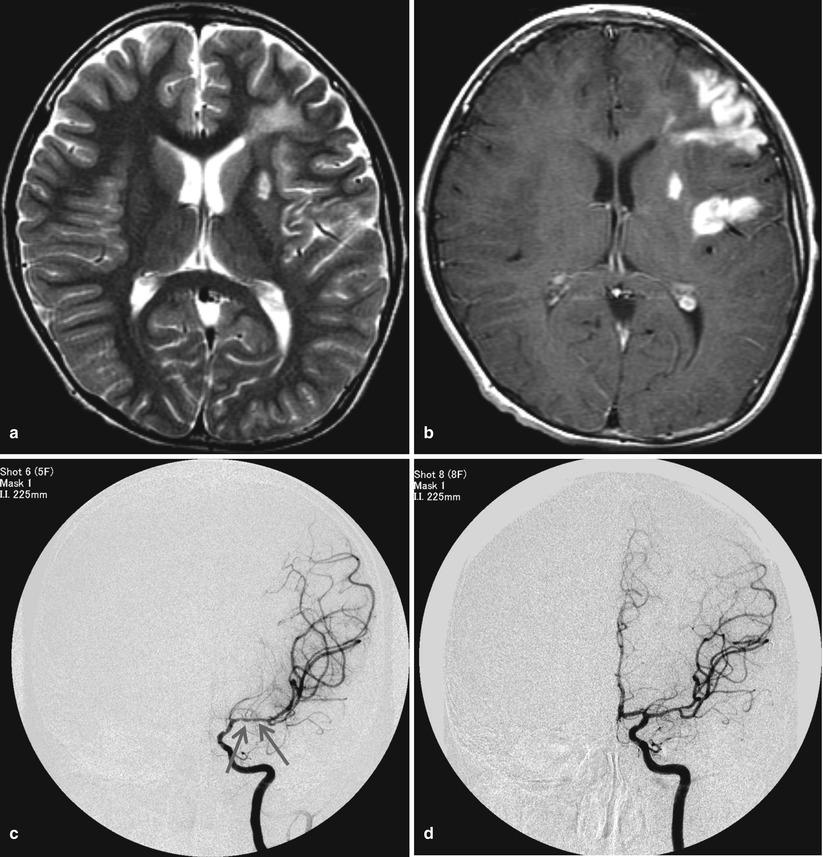
Fig. 3.10
An 8-month-old boy with right-side weakness suspecting post-viral angiitis. (a) T2-weighted image shows high signals in the left frontotemporal lobe and putamen. (b) Gyriform enhancement of the frontotemporal lesion and putamen suggests infarction. (c) Left distal internal carotid artery (ICA) and proximal middle cerebral artery (MCA) show mild irregular narrowing (arrow). (d) Three-year follow-up arteriography shows improved irregularities with residual mild narrowing of the MCA
3.4.9 Enterovirus Infection
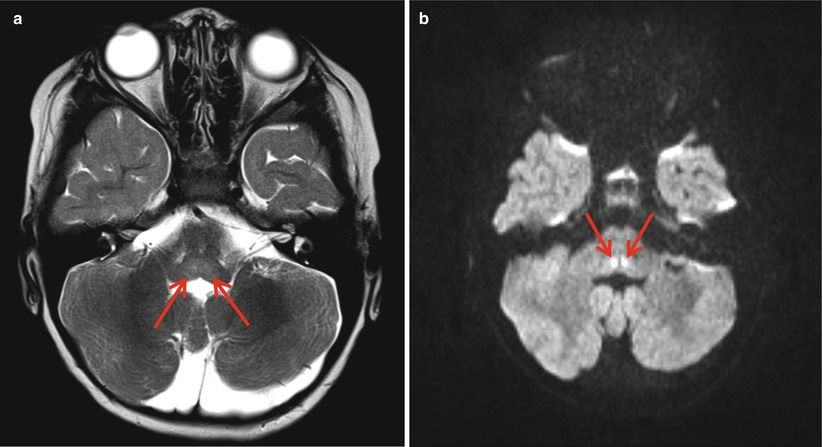
Fig. 3.11
A 3-year-old boy with fever and hand tremor 5 days after hand foot and mouth disease (HFMD). (a) T2-weight image shows subtle high signal in medulla (arrows). (b) Diffusion image reveals white matter tract lesions (arrows) in the dorsal medulla

Fig. 3.12
Rhombencephalitis after HFMD due to enterovirus. (a) T2-weighted image shows diffuse cerebellar high-intensity signals predominantly in the right hemisphere. (b) Postcontrast image shows diffuse cerebellar hemispheric enhancement along the folia