Fig. 13.1
Respiratory syncytial virus (RSV) infection in an 18-month-old boy. Frontal (a) radiograph demonstrates hyperaeration, perihilar peribronchial thickening, and areas of subsegmental atelectasis. Lateral view (b) shows depression of the diaphragm compatible with hyperaeration
13.5.2 Varicella Pneumonia
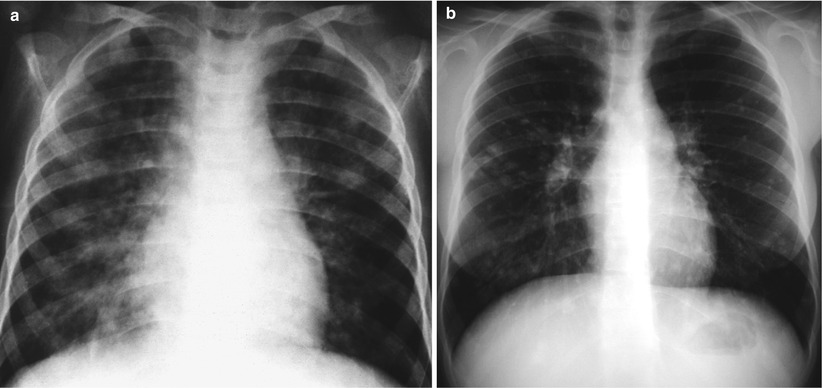
Fig. 13.2
Varicella pneumonia. Frontal chest radiograph of a 5-year-old boy showing multifocal patchy, nodular infiltrates throughout both lung fields (a). School requirement chest x-ray of a 15-year-old asymptomatic girl shows multiple, small, calcified nodules in both lung fields. The patient had varicella pneumonia 3 years prior (b)
13.5.3 SARS Infection
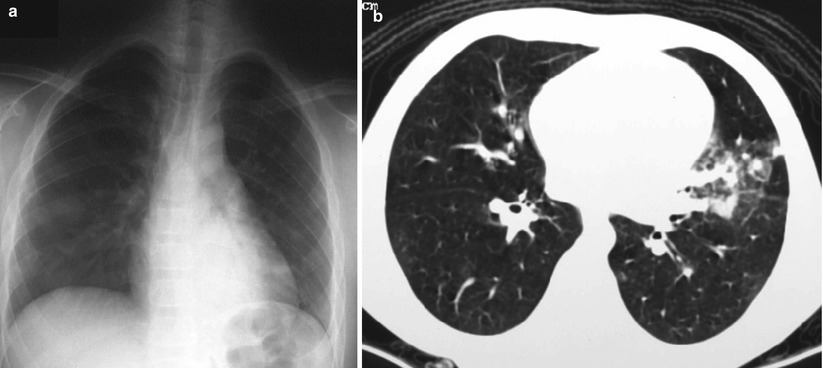
Fig. 13.3
SARS infection. Chest radiograph of a 13-year-old boy 3 days after the onset of fever shows ill-defined haziness in bilateral lower zones (a). An 8-year-old boy with confirmed SARS shows an area of mixed ground-glass opacity with consolidation in the lingula on HRCT (b) (Cases courtesy of Winnie CW Chu, MD, from Hong Kong)
13.5.4 Influenza AH1N1 Virus Pneumonia
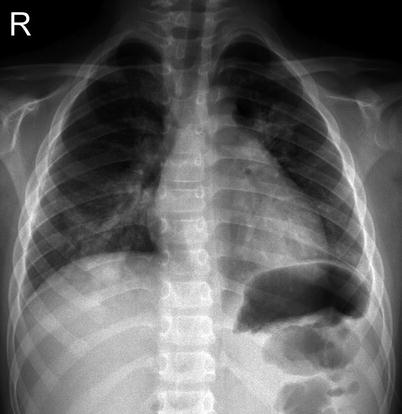
Fig. 13.4
AH1N1 virus pneumonia. Frontal chest radiograph shows generalized increase interstitial markings with multifocal patchy infiltrates (Case courtesy of Xanthe Marie Javier MD, from Philippines)
13.5.5 Postinfectious Bronchiolitis Obliterans

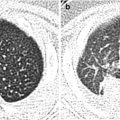
Fig. 13.5
Postinfectious bronchiolitis obliterans. High-resolution CT scan images in expiratory phase demonstrate the typical “mosaic perfusion” pattern
13.5.6 Swyer-James Syndrome
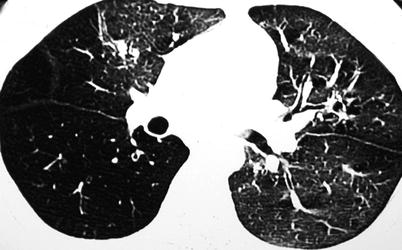
Fig. 13.6
Swyer-James syndrome in a 10-year-old girl. HRCT shows reduced attenuation and paucity of bronchovascular markings in the right lung (Case courtesy of Winnie CW Chu, MD, from Hong Kong)
13.5.7 Bacterial Pneumonia
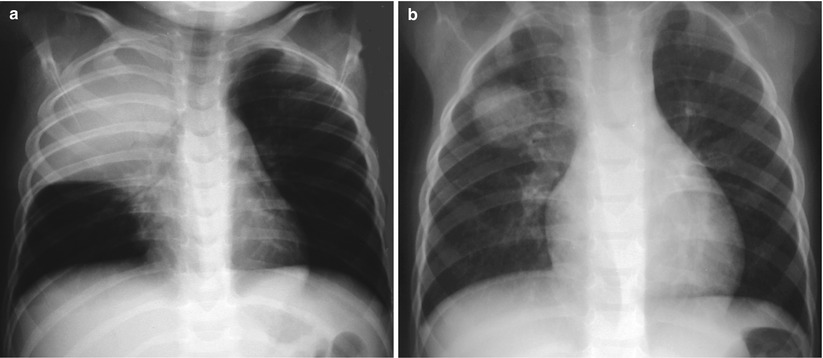
Fig. 13.7
Bacterial pneumonia. Chest radiographs of a 3-year-old girl with high fever, cough, and leukocytosis (a) demonstrate complete opacification of the right upper lobe. Image (b) shows a round, mass-like consolidation compatible with round pneumonia
13.5.8 Parapneumonic Fluid Collection: CT Finding

Fig. 13.8
Parapneumonic fluid collection on CT scan. Image demonstrates right-sided pleural fluid with thick enhancement of both visceral and parietal pleura
13.5.9 Parapneumonic Fluid Collection: Ultrasound Finding
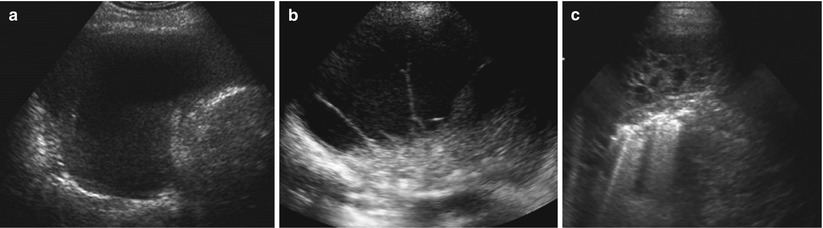
Fig. 13.9
Parapneumonic fluid collections on ultrasound. Simple effusion showing anechoic fluid without septations (a). Complicated fluid collection with thin septations and proteinaceous debris (b). Multiloculated fluid collection with thick septations and thickened pleural lining, compatible with fibrothorax (c)
13.5.10 Necrotizing Pneumonia
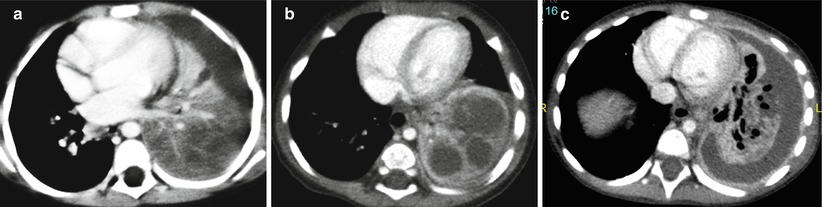
Fig. 13.10
Necrotizing pneumonia on CT. Left lower lobe consolidation showing diminished perfusion at the posterior region (a). Evolution of lung ischemia with development of multiple fluid-filled cavities (b). Cavitary necrosis of the consolidation with bronchopleural fistula and parapneumonic fluid (c)
13.5.11 Lung Abscess

Fig. 13.11
Lung abscess. Chest radiograph of a 7-year-old boy with cough and high fever reveals a large abscess with air–fluid level and thick irregular border in the right mid-lung. Notice other smaller abscess inferior to the primary lesion
13.5.12 Pneumatocele

Fig. 13.12
Pneumatocele. A 6-month-old boy recovering from Staphylococcus pneumonia reveals thin-walled cysts in the right mid-lung field and bibasilar regions
13.5.13 Bronchiectasis

Fig. 13.13
Bronchiectasis. Axial HRCT image showing thick-walled, dilated bronchi with diameters wider than the adjacent pulmonary arteries
13.5.14 Pertussis

Fig. 13.14
Pertussis. Chest radiograph of an 18-month-old boy showing right hilar adenopathy with streaky perihilar infiltrates obscuring the cardiac shadow (shaggy heart) (Case courtesy of Marion O. Sanchez, MD, from Manila, Philippines)
13.5.15 Mycoplasma Pneumonia
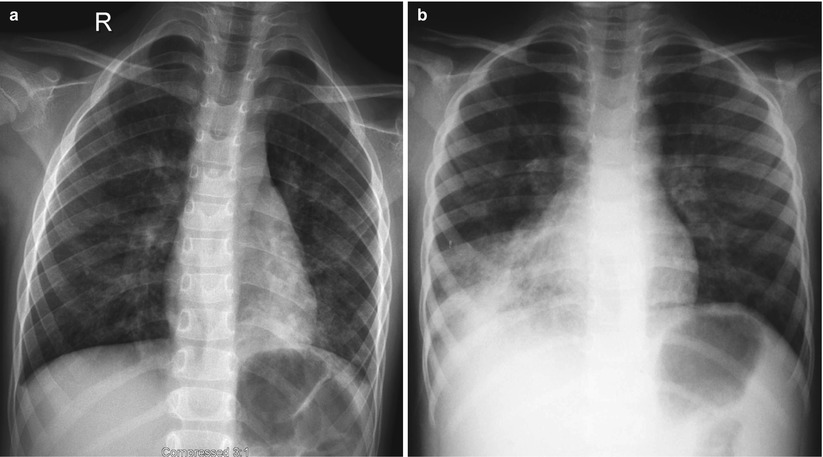
Fig. 13.15
Variable imaging pattern of Mycoplasma pneumonia. Chest x-ray of a 10-year-old boy (a) demonstrates generalized increase interstitial marking with scattered patchy areas of opacity. Another patient diagnosed with Mycoplasma infection demonstrating patchy consolidation on the right middle and lower lobes (b)
13.5.16 Chlamydia Pneumonia

Fig. 13.16
Chlamydia pneumonia. Radiograph of an afebrile 2-week-old girl with dry cough shows bilateral hyperaeration and diffuse interstitial infiltrates, appearing coalescent on the right
13.5.17 Tuberculosis: Primary TB
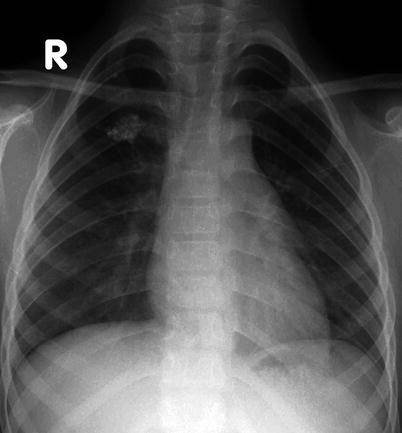
Fig. 13.17
Primary TB infection. An asymptomatic 7-year-old boy had a chest x-ray as a school requirement, which reveals a calcified granuloma on the right upper lobe. This corresponds to a calcified Ghon focus, a sign of TB infection
13.5.18 Tuberculosis: Primary TB
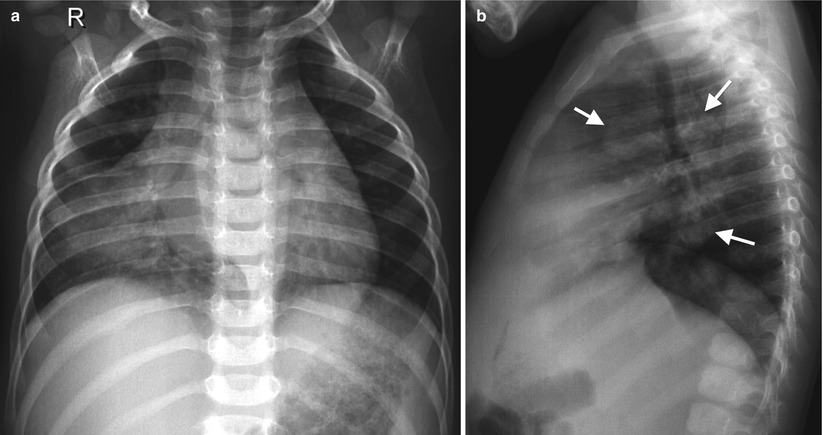
Fig. 13.18
Primary TB disease. Chest radiographs of a 2-year-old girl with chronic cough and fever showing dense right middle lobe consolidation on the frontal view (a) and extensive lymphadenopathy (white arrows) on the lateral view (b)
13.5.19 Tuberculosis: Progression of Ghon Focus
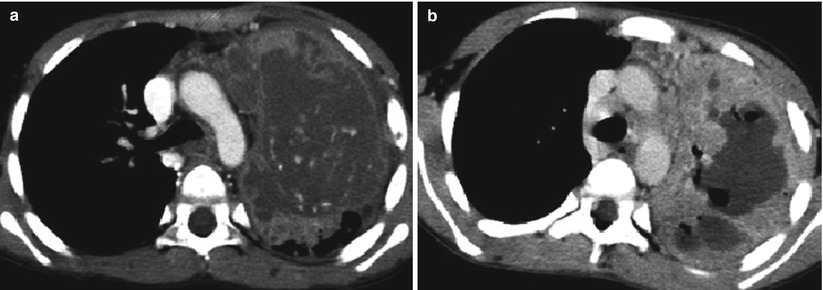
Fig. 13.19
Progression of Ghon focus. CT scan images from two different patients showing advanced progression of lung parenchymal disease from dense consolidation with ischemic changes (a) and cavitary necrosis with cyst formation (b)
13.5.20 Tuberculosis: Progression of Lymph Node Disease
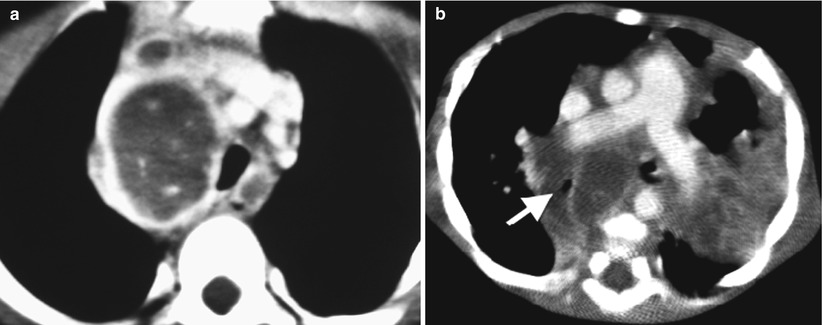
Fig. 13.20
Progression of lymph node disease. Image (a) demonstrates an enlarged right paratracheal lymph node effacing the trachea, with central hypoattenuation and peripheral contrast enhancement. Image (b) shows extensive subcarinal lymph nodes effacing the bronchi, especially the right mainstem bronchus (white arrow)
13.5.21 Miliary TB
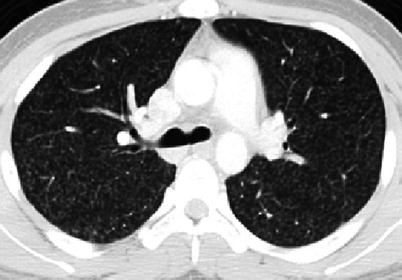
Fig. 13.21
Miliary TB. Axial CT image showing small (1–2 mm), uniform nodular densities scattered throughout both lungs compatible with disseminated TB disease
13.5.22 Reactivated TB

Fig. 13.22




Reactivation TB. Chest radiograph of a 13-year-old boy with chronic cough and shortness of breath showing fibrotic changes, pleural thickening, and volume loss in the right lung
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
