Fig. 16.1 Flowchart for the diagnosis and differential diagnosis of diseases that may affect the spinal cord.
Intramedullary processes cause variable neurologic symptoms that can range from mild sensory disturbances to a complete spinal cord lesion. ▶ Table 16.1 reviews possible intramedullary diseases and their imaging appearance on MRI.
Disease | T2w signal | T1w signal | Enhancement | Location | Typical findings |
Multiple sclerosis | Hyperintense | Isointense | In ca. 50% of cases | Often peripheral and posterolateral Cervical spine affected more often than thoracic spine | <2 segments <1/2 of cord cross-section 50% multifocal Cerebral lesions |
Neuromyelitis optica (Devic’s syndrome) | Hyperintense | Isointense | Variable | Cervical and thoracic spine | 3 segments or more 80% also have brain lesions, usually asymptomatic |
Transverse myelitis | Hyperintense | Iso- or hypointense | Variable | Central in cervical or thoracic spine | >2 segments >2/3 of cord cross-section |
Funicular myelosis (vitamin B12 deficiency) | Hyperintense | Iso- or hypointense | None | Dorsal columns Cervical or thoracic spine | >2 segments Typical appearance |
Spinal infarction | Hyperintense | Iso- or hypointense | None | Central | Possible small mass, often H-shaped (“snakebite”), acute onset Demarcated within 24 h in c.50% of cases |
Dural arteriovenous fistula | Hyperintense | Hypointense | None (congested veins enhance!) | Central Often located in lower thoracic spine | Perimedullary flow voids (3-mm slices) |
Tumor | Hyperintense | Hypointense | Intense | Central | Possible syrinx surrounding the mass |
Cavernous hemangioma | Mixed (popcorn) | Mixed | Little or none | Usually central | Hemosiderin rim T2*w images very sensitive |
Syrinx | Hyperintense | Hypointense | None | Central | Underlying cause (tumor, Chiari I, trauma) |
Myelitides are inflammations of the spinal cord that may affect the gray matter (poliomyelitis) or white matter (leukomyelitis). Inflammation involving the full cross-section of the cord is called “transverse myelitis.” These definitions have not been used consistently or uniformly in the literature. Some authors use “acute transverse myelitis” as a collective term for almost all nonneoplastic intramedullary diseases. The main reason for such inconsistency is that the MRI findings are relatively nonspecific despite the varied causes—a consequence of the limited range of responses that the spinal cord can have to various diseases. The distribution pattern of the lesions on MRI can sometimes narrow the differential diagnosis. In many cases, however, the cause of a lesion ultimately remains unexplained.
Even so, diagnostic imaging still plays an important role in these patients because it can exclude cord compression and can sometimes identify treatable causes that underlie nonspecific neurologic symptoms. Thus, the presence of central, nonenhancing spinal cord edema should always prompt a search for a dural arteriovenous fistula. Exclusive involvement of the dorsal columns is typical of funicular myelosis due to vitamin B12 deficiency.
Extradural processes such as spondylodiskitis and epidural abscesses usually develop in the wake of other infectious diseases, especially in immunocompromised patients, in diabetics, or as an iatrogenic process following intervertebral disk surgery or infiltration. The dominant findings in these cases are fever, back pain, and an elevated erythrocyte sedimentation rate (ESR).
In the sections that follow, we describe the more common diseases in considerable detail while reviewing less common diseases more briefly.
16.2 Intramedullary Space
This section deals with inflammatory diseases that show primary involvement of the spinal cord. The MRI findings in these diseases are not very specific, but in many cases the differential diagnosis can be narrowed by also imaging the brain. The brain and spinal cord are composed of the same tissues and are bathed in CSF. As a result, intramedullary lesions often coexist with intracerebral changes, and the differential diagnosis is advanced by “looking upward” from the spine.
Note
“Looking upward” (concurrent brain imaging) can be rewarding in patients with presumed inflammatory diseases of the spinal cord.
An initial search for intramedullary lesions can generally be accomplished with a sagittal T2w sequence. More recent studies suggest that STIR sequences may provide a better detection rate of intramedullary lesions than a pure T2w sequence. If these sequences reveal an abnormal or suspicious finding, the protocol should then be expanded to include T1w sequences, additional planes, and intravenous contrast administration.
Tips and Tricks
In the MRI of intramedullary lesions, do not use fat suppression after contrast administration, as this leads to increased image noise that could obscure subtle findings. On the other hand, fat suppression is very helpful for extramedullary and extradural processes to facilitate the detection of any enhancing areas in the hyperintense fat.
The following sections are subdivided into demyelinating diseases and transverse myelitis is solely for convenience. Often these entities cannot be positively distinguished from one other on the basis of imaging findings.
16.2.1 Multiple Sclerosis and Other Demyelinating Diseases
16.2.1.1 Multiple Sclerosis
Definition Multiple sclerosis is a chronic, inflammatory, demyelinating autoimmune disease of the central nervous system in which lesions develop at various sites in the central nervous system (CNS) and at different times.
Epidemiology Multiple sclerosis is the most common inflammatory disease of the CNS and the second most common neurologic disease after epilepsy. Its prevalence in Germany is approximately 80:100,000 population per year, with approximately 100,000 total cases at the present time. Women are predominantly affected by about a 2:1 ratio. In 75% of patients the disease is manifested between 20 and 40 years of age.
Clinical manifestations Patients typically present clinically with recurrent motor and/or sensory deficits in various anatomic regions. Spinal involvement correlates with clinical symptoms somewhat better than intracerebral lesions and presents mainly with sensory disturbances. The most common initial presenting symptom is retrobulbar neuritis.
Pathogenesis The pathogenesis of multiple sclerosis is not yet fully understood. Presumably it involves an autoimmune process leading to inflammatory demyelination of the white matter in the brain and spinal cord. The resulting defects are called “inflammatory lesions” or “plaques.” Histologically, early lesions consist of myelin disruption that spares the axons and is accompanied by microglial proliferation. Further progression is characterized by additional loss of myelin and oligodendrocytes as well as fatty infiltration. There is an associated proliferation of astrocytes and perivascular inflammation, which may also involve the gray matter but spares the neuronal cell bodies for some time. Eventually the axons are also affected, leading to Wallerian degeneration. The clinical presentation shows only a slight correlation with lesions detectable by MRI.
MRI findings Spinal cord lesions are found in up to 80% of patients with CNS involvement. The cervical cord is affected in approximately 60% of cases. Isolated involvement of the spinal cord is found in approximately 10 to 20% of multiple sclerosis patients. An absence of intracranial lesions therefore does not exclude multiple sclerosis. Spinal multiple sclerosis plaques appear on T2w images as hyperintense intramedullary lesions located predominantly in the white matter of the spinal cord, usually without an associated mass effect. Imaging in the acute stage may show moderate swelling of the spinal cord due to perifocal edema. A decrease in cord volume may be found in the late chronic (“burned out”) stage. The lesions are frequently located in the posterolateral white matter, but any other intramedullary sites may be involved. Longitudinal involvement usually spans more than one segment. Two or more intramedullary lesions are present in approximately one-half of cases. The best survey view is obtained with sagittal T2w images ( ▶ Fig. 16.2) or STIR images, which are supplemented in positive cases by axial T2w images of the affected region. Axial images clearly demonstrate the relative involvement of the gray and white matter and can positively distinguish true lesions from plane-of-section effects. Often the lesions are not visualized on unenhanced T1w images; rarely they appear as faint hypointensities. As with cerebral lesions, T1w images with gadolinium contrast show enhancement in approximately one-half of symptomatic patients. The inflammatory processes that surround multiple sclerosis lesions may lead to the spread of edema and possible enhancement in the adjacent gray matter. This can make the lesions difficult to distinguish from a glial tumor in some cases. Especially with solid lesions, spinal MRI should be supplemented by an MRI examination of the brain, which will reveal typical multiple sclerosis lesions in 80 to 90% of patients, thereby supporting the diagnosis.

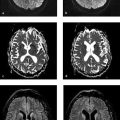
Fig. 16.2 Multiple sclerosis in a 22-year-old woman with a 6-week history of sensory disturbances in her right arm. No other symptoms were present. CSF was positive for oligoclonal bands. (a) Axial FLAIR sequence of the brain demonstrates multiple hyperintense lesions. (b) Axial DIR sequence of the brain. The lesions are depicted in higher contrast. (c) Sagittal T2w image of the cervical spine demonstrates multiple hyperintense lesions. Each of the lesions spans no more than one vertebral body height. (d) Sagittal T1w sequence after contrast administration. Individual lesions show marked enhancement.
Note
Between 80% and 90% of patients with spinal involvement by multiple sclerosis also have intracranial lesions.
This is particularly true when we apply the criteria first published by McDonald et al in 2001 and most recently updated in 2010. In patients with only a few, nonspecific cerebral white-matter lesions, the detection of concomitant spinal lesions increases the probability of multiple sclerosis. On the other hand, multiple sclerosis can be excluded with high confidence in symptomatic patients if imaging (with proper technique) does not detect either cerebral or spinal lesions.
16.2.1.2 Acute Disseminated Encephalomyelitis
Definition Acute disseminated encephalomyelitis (ADEM) is a rare, acute inflammatory demyelinating disease of the CNS which typically develops within the first 3 weeks after a viral infection or vaccination and runs a monophasic course.
Epidemiology Unlike multiple sclerosis, ADEM affects both sexes equally and may occur at any age. Only the brain is affected in most cases; spinal lesions are much rarer than in multiple sclerosis.
Clinical manifestations The disease has an acute onset and is often rapidly progressive. The mortality rate is as high as 30%. Symptoms may include paralysis, visual disturbances, sensory deficits, and signs of increased intracranial pressure (headache, vomiting, papilledema).
Pathogenesis The cause of ADEM is not fully understood. Like multiple sclerosis, it causes demyelination in affected regions. This process is often associated with multifocal inflammatory lesions that affect the perivenous regions and lead to perivenous and subpial demyelination. Spinal cord involvement is less common than in multiple sclerosis.
MRI findings In contrast to multiple sclerosis, the changes often affect the entire cross-section of the spinal cord. The MRI findings in these cases are nonspecific and are indistinguishable from transverse myelitis unless correlated with clinical findings and intracerebral lesions ( ▶ Fig. 16.3). Hemorrhagic changes are occasionally found in cases with a fulminating course, but they are not specific for ADEM. All lesions are of the same age due to the monophasic course of the disease.

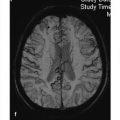
Fig. 16.3 ADEM in a 15-year-old girl with headaches and visual impairment 1 week after a viral infection. She went on to develop left hemiparesis and decreased alertness. CSF examination showed pleocytosis and signs of intrathecal IgG synthesis. (a) Axial FLAIR image of the brain shows a sharply circumscribed hyperintensity in the right frontal region. (b) Axial T1w image of the brain after contrast administration shows marked ring enhancement around the right frontal lesion. (c) Sagittal T2w image shows intramedullary hyperintensity at the level of the T10 and T11 vertebral bodies. (d) Sagittal T1w image after contrast administration shows no evidence of enhancement. (e) Axial T2w image at the level of the lesion. The hyperintensity involves the whole cross-section of the spinal cord.
16.2.1.3 Neuromyelitis Optica (Devic’s Syndrome)
Definition Neuromyelitis optica is another demyelinating disease, characterized by demyelination of the optic nerve leading to visual impairment or blindness. There is associated transverse myelitis, which often takes a fulminating course. For many years neuromyelitis optica was considered a special form of multiple sclerosis, but today most experts classify it as a separate entity.
Epidemiology The prevalence in Europe is 1 to 4:100,000 population per year.
MRI findings and clinical manifestations Spinal MRI findings are more pronounced than in multiple sclerosis. The lesions usually involve more than three segments, and swelling of the spinal cord is often noted over the involved levels. In this respect the spinal MRI findings closely resemble the changes in ▶ transverse myelitis. A diagnosis of neuromyelitis optica requires clinical correlation, i.e., visual impairment with concurrent or slightly delayed onset of spinal symptoms. Cranial MRI findings in typical cases do not meet the diagnostic criteria for multiple sclerosis ( ▶ Fig. 16.4). Optic nerve damage appears as isolated hyperintensity confined to the optic nerves in coronal fat-saturated T2w images.

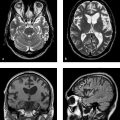
Fig. 16.4 Neuromyelitis optica in a 25-year-old woman with left-sided optic neuritis and quadriparesis. CSF examination showed pleocytosis. Serum test was positive for aquaporin antibodies. (a) FLAIR image of the brain shows a small, nonspecific white-matter hyperintensity in the left frontal region. (b) Sagittal T2w image of the cervical spine shows hyperintensity extending along the spinal cord from the C1 to C5 levels. (c) Axial T1w image after contrast administration shows circumscribed enhancement on the right side. (d) Sagittal T1w image after contrast administration. The T2w hyperintensity in panel b shows partial enhancement.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


