Intralobar Sequestration
Jud W. Gurney, MD, FACR
Key Facts
Terminology
Pulmonary sequestration represents nonfunctioning lung tissue separated from normal lung
Receives its blood supply from systemic artery
Intralobar sequestration (90%)
Extralobar sequestration (10%)
Imaging Findings
95% lower lobes
Persistent left-sided inferior paraspinal opacity with history of recurrent pneumonia
Cystic-bronchiectatic form
Pseudotumor form
Emphysematous form
Lung bordering sequestration often hyperinflated or emphysematous
Systemic artery
Origin: Thoracic aorta (75%)
Origin: Abdominal aorta (20%)
Artery can measure up to 1 cm in diameter, often shows intimal calcification
Venous drainage via inferior pulmonary vein
Top Differential Diagnoses
Extralobar Sequestration
Transpleural Systemic-Pulmonary Artery Anastomoses (Pseudosequestration)
Chronic Pneumonia/Lipoid Pneumonia
Postobstructive Pneumonia/Central Bronchial Neoplasm
Clinical Issues
Persistent opacification in same portion of lower lobe should raise suspicion for diagnosis
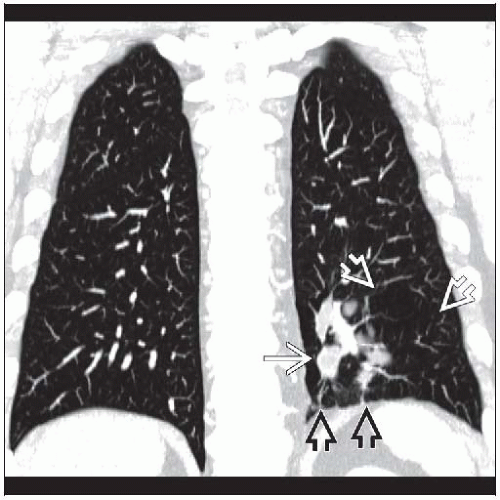 Coronal CECT reconstruction shows sequestration  surrounded by hyperlucent lung surrounded by hyperlucent lung  and fed by arteries and fed by arteries  crossing the hemidiaphragm. crossing the hemidiaphragm. |
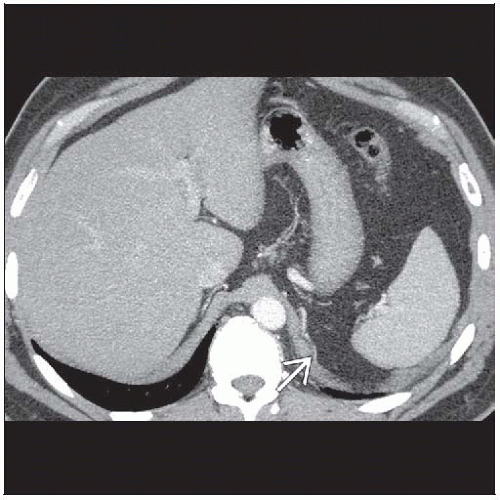 Axial CECT shows a small artery  that had arisen from the aorta adjacent to the hemidiaphragm. that had arisen from the aorta adjacent to the hemidiaphragm. |
TERMINOLOGY
Definitions
Malinosculation: Congenital abnormal connection of 1 or more of 4 components of lung (airways, arterial supply, venous drainage, and parenchyma)
Pulmonary sequestration represents nonfunctioning lung tissue separated from normal lung
Receives its blood supply from systemic artery
Normal communication with bronchi lost
2 major forms
Intralobar sequestration (90%)
Shares visceral pleura of normal lung
Extralobar sequestration (10%)
Has separate pleura from normal lung
Communicating bronchopulmonary foregut malformation is uncommon form of sequestration, usually seen with extralobar type
IMAGING FINDINGS
General Features
Best diagnostic clue: Persistent left-sided inferior paraspinal opacity with history of recurrent pneumonia
Patient position/location
95% lower lobes
Left lower lobe (65%), right lower lobe (55%)
Posterior basal segment > medial basal segment
Size: Variable, but cystic lesions often quite large
CT Findings
Sequestrum characteristics
Cystic-bronchiectatic form
Cysts may be single or multiple
Cysts contain fluid or air (air-fluid levels)
Cystic form often quite large
Pseudotumor form
Spiculated mass mimics bronchogenic carcinoma
Homogeneous or inhomogeneous
May enhance with intravenous contrast
Emphysematous form
Emphysematous lung only
Lung bordering sequestration often hyperinflated or emphysematous
Systemic artery
Identification from aorta is diagnostic
Artery can measure up to 1 cm in diameter, often shows intimal calcification
Nonvisualization of systemic artery does not exclude diagnosis
Occasionally, multiple small arteries supply sequestration (15-20%)
Systemic arterial supply without sequestration (known as Pryce type 1 sequestration)
Anomalous artery only
Prominent inferior pulmonary vein
Absence of interlobar artery distal to origin superior segmental artery
Normal bronchial system (absent sequestrum)
Pulmonary artery supply normal or absent
Venous drainage via inferior pulmonary vein
Calcification and effusions uncommon
Radiographic Findings
Inferior paraspinal mass or opacity located in posterior basal segment adjacent to diaphragm
Margins may be either sharp, lobulated, or ill-defined
Concurrent volume loss common
1/3 of cystic sequestrations contain air or air-fluid levels
Localized emphysema without consolidation or fluid is well described but uncommon
Chronic or recurrent bacterial pneumonia
May decrease in size with antibiotic therapy, but will not resolve
Pleural effusion (4%) and calcifications rare
MR Findings
Excellent depiction of complex cystic, solid, and fibrotic components
Cysts have variable signal depending on fluid
Often higher signal on T2WI sequences
Hemorrhage within lesion represented by high signal on both T1WI and T2WI sequences
Angiographic Findings
Traditional method of diagnosis but now replaced by CT angiography
Used to embolize feeding arteries
Origin of feeding artery
Thoracic aorta (75%)
Abdominal aorta (20%)
Intercostal artery (5%)
Multiple (16%)
Vessels < 3 mm likely 1 of multiple supplying arteries
95% have pulmonary venous drainage
5% systemic venous drainage, usually via azygos, hemiazygos, superior vena cava, or intercostal routes
DIFFERENTIAL DIAGNOSIS
Extralobar Sequestration
Congential lesion, often presents in 1st 6 months
Completely distinct entity from intralobar form
Associated with other congential anomalies
Systemic arterial supply from aorta
Drainage into systemic veins (80%), not pulmonary
Invested in own pleural lining, separated from normal lung
Essentially accessory lung
Located on left in 90%, although may lie within or below diaphragm
Transpleural Systemic-Pulmonary Artery Anastomoses (Pseudosequestration)
Systemic arterial supply across pleural adhesions
Seen with pulmonary artery stenosis, less perfused upper lobes fed by intercostal arteries
Pleural arterial blush not seen with sequestration
Vessels often tangled on surface of mass
Placental Transmogrification of the Lung
Chronic Pneumonia/Lipoid Pneumonia
Chronic consolidation in lower lobe, such as lipoid pneumonia
No aberrant arterial supply
Arteriovenous Malformation, Pulmonary
Single or multiple nodulesRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



