Introduction to Cardiac Imaging
Ramesh S. Iyer, MD
Mark R. Ferguson, MD
LEARNING OBJECTIVES
1. Discuss the various options for pediatric cardiac imaging, including each modality’s strengths and drawbacks.
2. Generate a list of features to assess when interpreting chest radiographs for children with suspected congenital heart disease.
3. Identify features of pulmonary arterial overcirculation or “shunt vascularity.”
4. Recognize cardiomegaly on chest radiography for young children.
5. Identify a right-sided aortic arch and its implications for congenital heart disease.
6. Recognize situs abnormalities and their implications for congenital heart disease.
INTRODUCTION
Gone are the days when congenital heart disease was routinely identified on chest radiographs and characterized by cardiac angiography. Cardiac imaging has been revolutionized by echocardiography, cardiac CT, and MR. These modalities offer exquisite structural detail and functional data by which the interventional cardiologist or cardiac surgeon can make reliable management decisions. It is important for the radiologist to understand the role of radiography and fundamentals of these cross-sectional modalities to optimize the diagnostic workup of these lesions.
ECHOCARDIOGRAPHY
Echocardiography is the primary cardiac imaging modality in children. Echocardiography alone is sufficient for characterizing most cardiac anomalies before definitive treatment. These examinations may be performed using either a transthoracic or transesophageal approach. High-resolution ultrasound transducers, portability, and excellent acoustic windows have increased the effectiveness of pediatric echocardiography.1 As with all ultrasound studies, a major advantage of echocardiography is its lack of ionizing radiation, while operator dependence is a potential limitation. Echocardiography is highly efficient at delineating intracardiac morphology and function. There is less success, however, with detailing extracardiac vasculature.1,2 CT and MR serve as useful adjunct modalities when extracardiac vascular pathology is suspected.
Gray-scale imaging and color and spectral Doppler interrogation are performed with echocardiography (Fig. 9.1). Assessment of ventricular systolic and diastolic function is achieved by measuring chamber dimensions at various points in the cardiac cycle. Color Doppler is helpful for screening for septal defects and valvular stenosis or regurgitation. Spectral Doppler is applied to all cardiac valves, the aortic isthmus, and any septal defects to further evaluate and quantify flow dynamics.2
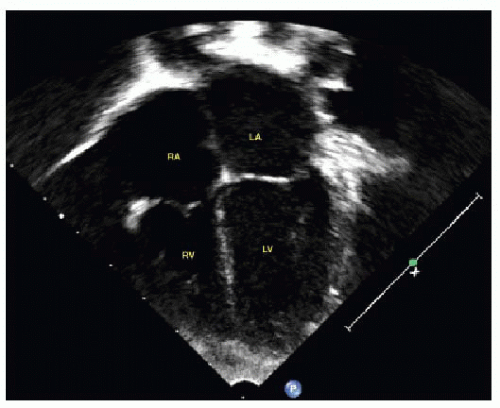 FIG. 9.1 • Echocardiogram apical 4-chamber view demonstrating normal anatomy of the atria (RA and LA) and ventricles (RV and LV). Echocardiography remains the primary imaging modality for congenital heart disease. |
CARDIAC CT ANGIOGRAPHY
The advent of multidetector computed tomography (MDCT) to pediatric cardiovascular imaging brought several benefits. Compared to echocardiography, catheter angiography, and MR, CT provides the most comprehensive evaluation of the thorax. Acquired disorders of the lungs and airways, including the effects of vascular rings and slings, can be imaged in great detail. Sedation is less frequently needed than other modalities, with newer technology featuring scan times of less than one second. CT is less inhibited by metal artifact than is MR and is more accommodating of monitoring devices. On the other hand, two drawbacks with cardiac CT are the incorporation of ionizing radiation and iodinated contrast media.3, 4 and 5
Pediatric cardiac CT examinations often require more handson scan parameter manipulation by the radiologist than adult cardiac studies. The goal of optimizing image quality is counterbalanced by the need to minimize radiation dosage (Fig. 9.2). CT studies may utilize either retrospective or prospective ECG gating or be performed as a nongated study. Prospective ECG gating is often preferred in children due to reduced radiation with preserved image quality.3,5 While fast heart rates of young children and particularly unsteady rhythms remain potential limiting factors for CT scans, the newer generation of fast wide-area multidetector scanners (256 or 320 slice) promises to overcome most of these obstacles. Scan collimation is less than 1 mm, with a pitch of less than 1 for ECG-gated examinations and 1 to 1.5 for nongated studies.4,5 Thin detector configurations allow for optimal image reconstructions. MDCT examinations provide multiplanar, volume, and curved (coronary artery) reconstructions.3 In general, using optimized scanning parameters, cardiac CT angiograms may be performed with a radiation dosage that is similar to or less than a standard chest CT.5 Examinations performed with a retrospective technique can also provide functional information (e.g., ejection fraction) but at the cost of increased radiation dose.
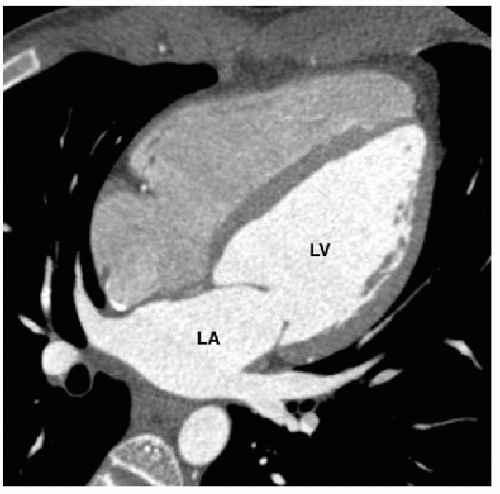 FIG. 9.2 • ECG-gated cardiac CT reformatted into a fourchamber view demonstrating normal anatomy. The contrast bolus timing was optimized to predominantly opacify the left heart (LA, left atrium; LV, left ventricle) for this examination. CT can provide exquisite high-resolution detail of anatomic structures. |
CARDIAC MR
Cardiac MR has also transformed imaging of congenital heart disease. It offers precise anatomic detail along with a quantitative functional evaluation. The absence of ionizing radiation is a significant advantage. MR is generally more expensive than other modalities, with the possible exception of cardiac angiography. While sedation is often necessary for young children, newer techniques and sequences have decreased the need for prolonged anesthesia. Both preoperative and postoperative cardiac MR imaging may be performed, with the latter being more common. MR is also superior to echocardiography in assessing right ventricular function, which is one of the most common clinical questions to be answered.
Noncontrast sequences in cardiac MR can be divided into two categories. Spin echo pulse sequences, or “black-blood” imaging, are primarily used to define anatomy (Fig. 9.3). Double inversion recovery further nulls blood signal and accentuates the contrast resolution between the blood-filled lumen and the adjacent cardiac or vessel wall. Vascular morphology, cardiac chamber relationships, and airway and visceral anatomy are shown to great advantage. Spin echo sequences are performed with ECG gating, and either breath holding or multiaveraged free breathing techniques. Balanced steady-state free precession (b-SSFP) cine sequence is a type of gradient echo pulse sequence in which blood has a bright signal, termed “bright blood” imaging (Fig. 9.4). b-SSFP cine sequences are preferred for assessing cardiac motion and quantifying function and are really the workhorse for cardiac MRI examinations. Turbulent flow, such as across a septal defect, appears as a black jet against a background of white blood on a gradient echo sequence.1,6,7
MRI also has the ability to provide myocardial tissue characterization. T2-weighted images can demonstrate regions of myocardial edema/inflammation. This can be complemented with assessment for late gadolinium enhancement that can be seen in the setting of inflammation, infection, ischemia, and fibrosis. Newer techniques utilizing T1 mapping aim to further expand the role of MRI in tissue characterization.
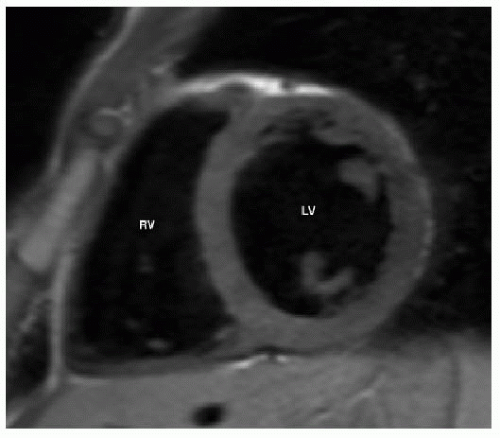 FIG. 9.3 • Black blood T1-weighted short-axis image through the mid aspect of the right and left ventricles (RV and LV). Black blood images can be used primarily to define anatomy. |
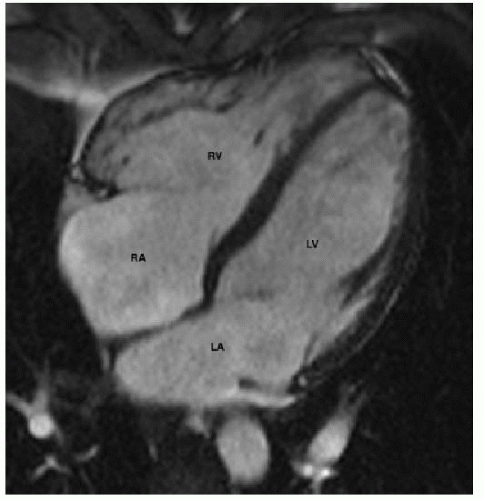 FIG. 9.4 • Bright blood (b-SSFP) 4-chamber view demonstrating normal anatomy of the atria (RA and LA) and ventricles (RV and LV). b-SSFP images are often obtained as cine sequences and are the workhorse for cardiac MRI functional assessment. |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


