1. List clinical and imaging features that raise suspicion for nonaccidental trauma.
2. Identify patients who may benefit from hepatic arterial embolization.
3. Recognize CT findings that might prompt emergent surgery in a child with blunt abdominal trauma.
4. Diagnose pancreatic injury based on CT findings.
5. Differentiate duodenal hematoma from perforation.
6. Recognize abdominal CT features of shock.
INTRODUCTION
Trauma is the leading cause of morbidity and mortality in children older than 1 year.1 Blunt abdominal trauma in children is relatively infrequent, accounting for approximately 2% to 8% of all trauma cases in children.2,3and4 However, published mortality rates are as high as 13% to 45%, with concomitant traumatic brain injury implied as the major factor in fatal cases.4,5and6 Intra-abdominal injuries from blunt trauma may be difficult to recognize clinically due to the inability of young patients to communicate effectively5,7 or due to loss of consciousness or altered mental status. The majority (approximately 80%) of children able to be assessed following trauma present with abdominal pain.8 Whereas victims of high-velocity injuries—for instance, motor vehicle accidents or falls from significant heights—tend to present immediately to medical centers for care, children injured by lesser insults or by nonaccidental trauma (NAT) often receive delayed care.4,7,9 In the pediatric population, differentiation between NAT and trauma becomes very important to ensure the future well-being of the child. The different patterns of injuries seen in these two distinct pediatric groups are discussed in this chapter as well as the appropriate diagnostic imaging for blunt abdominal trauma in the child.
NONACCIDENTAL TRAUMA
Diagnostic radiologists, along with our pediatric clinical colleagues, have a critical role in protecting children from maltreatment. It has been estimated that the rate of abuse is approximately 4.9 children per 1,000,10 and some studies show that up to 17% of hospital admissions for abdominal trauma in infants are attributable to NAT.11,12 Intra-abdominal injuries in children less than 4 years of age are more often caused by NAT than by accidents,4,7,9,13 and as mentioned above, the presentation of affected children to health care centers is more likely to be delayed than when a child is injured accidentally. Intra-abdominal injuries from NAT are often more severe than are those seen with accidental trauma, with higher rates of emergent surgical exploration5,11 and mortality2,5,14 in NAT cases. Risk factors for abdominal trauma due to NAT are the same as other types of injuries caused by NAT and include poverty, single-mother families, and male gender.11Table 18.1 summarizes the types of injuries that are specific for NAT.15
Different patterns of intra-abdominal injuries have also been observed in children presenting after NAT compared with accidental abdominal trauma. Solid abdominal organs are usually injured with high-velocity accidents such as motor vehicle accidents and falls from heights above 10 feet, with the whole-body inertia leading to a “burst injury” (Fig. 18.1). In contrast, there is a disproportionately high rate of injuries to the pancreas and hollow viscus organs caused by NAT, due to a direct impact to the abdomen (see Table 18.2; Fig. 18.2).4,8,9,14 The duodenum and proximal jejunum are the most commonly seen hollow viscus injuries in NAT victims, although stomach, bladder, and large bowel injuries have also been reported.13,16
The observed injuries must be assessed in the context of the reported mechanism of injury. In cases of inflicted trauma, the injuries are commonly inconsistent with the type of trauma reported by the infant or child’s care provider.7,17 For instance, a low-level fall is a frequently provided explanation in cases of abuse; however, hollow viscus injury is exceedingly rare in such falls.16,18 A retrospective literature review by Huntimer et al.19 summarized that in 312 reported cases of small intestinal perforations, none was caused by a fall on stairs, and in 677 reported cases of falls on stairs, none resulted in intraabdominal injuries. While there is undoubtedly overlap in the intra-abdominal injury patterns of accidental and inflicted trauma in the pediatric patient, NAT should be seriously considered in patients less than 4 years of age, in those with a pancreatic injury or hollow viscus injury, and in cases where the stated mechanism of injury is discordant with the severity of injuries.
Table 18.1 IMAGING FINDINGS HIGHLY SPECIFIC FOR NONACCIDENTAL TRAUMA IN INFANTS AND TODDLERS.
System
Highly Specific
Worrisome
Skeletal
Metaphyseal fractures
Rib fractures
Any fracture in infants and toddlers that is discordant with the clinical history
Skull fractures that are depressed, multiple, bilateral, or crossing sutures
Central nervous system
Subdural hemorrhage
Subarachnoid hemorrhage
Diffuse axonal injury
Parenchymal contusion
Cerebral edema
Stroke
Visceral injury
Small bowel injury
Pancreatic injury
Spleen, liver, renal, or urinary bladder
From Lonergan GJ, Baker AM, Morey MK, et al. From the archives of the AFIP. Child abuse: radiologic-pathologic correlation. Radiographics. 2003;23(4):811-845.
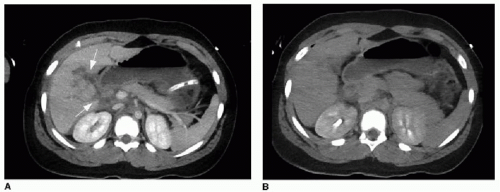
FIG. 18.1 • A 10-year-old motor vehicle accident victim with grade IV liver laceration. Abdominal CT study performed in portal venous phase (A) and delayed phase (B) shows a complex set of nonenhancing linear areas (arrows in A) extending to the porta hepatis, consistent with a complex hepatic laceration (grade IV). Delayed imaging demonstrates no contrast extravasation. This type of “burst imaging” is typical of high-impact accidents.
Table 18.2 LIVER INJURY SCALE (1994 REVISION)
Grade
Description
Definition
I
Hematoma
Subcapsular, <10% surface area
I
Laceration
Capsular tear, <1 cm parenchymal depth
II
Hematoma
Subcapsular, 10%-50% surface area; intraparenchymal, <10 cm in diameter
II
Laceration
1-3 cm parenchymal depth, <10 cm in length
III
Hematoma
Subcapsular, >50% surface area or expanding; ruptured subcapsular or parenchymal hematoma; intraparenchymal hematoma >10 cm or expanding
III
Laceration
>3 cm parenchymal depth
IV
Laceration
Parenchymal disruption involving 25%-75% of hepatic lobe or 1-3 Couinaud segments within a single lobe
V
Laceration
Parenchymal disruption involving >75% of hepatic lobe or >3 Couinaud segments within a single lobe
V
Vascular
Juxtahepatic venous injuries; that is, retrohepatic vena cava/central major hepatic veins
VI
Vascular
Hepatic avulsion
Modified from Moore EE, Cogbill TH, Jurkovich GJ, et al. Organ injury scaling V: spleen and liver (1994 revision). J Trauma. 1995;38:323-324.
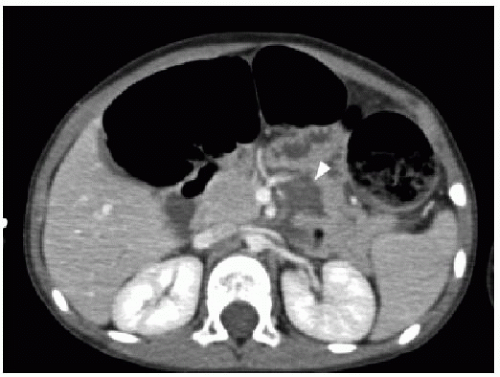
FIG. 18.2 • Nonaccidental (inflicted) trauma. Abdominal CT study performed on a 1-year-old infant in portal venous phase through the pancreas demonstrates a broad nonenhancing area through the midportion of the pancreas (arrowhead), consistent with pancreatic fracture.
DETECTION OF INJURY AND IMAGING
Assessment by clinicians of the injured child in the emergency department requires a stepwise approach that primarily evaluates for immediately life-threatening injuries and then secondarily searches for less severe injuries. Upon initial presentation at an experienced trauma center, if intra-abdominal injury is suspected, focused assessment by sonography for trauma (FAST) may be utilized as an initial diagnostic tool for detection of hemoperitoneum.20,21 The technique simply involves a rapid assessment of the four quadrants of the abdomen and the paracolic gutters by ultrasound to identify free fluid (Fig. 18.3). The use of FAST is controversial in children, and a thorough meta-analysis including review of 25 studies and 3,838 children published by Holmes et al.22 indicates that abdominal ultrasonography in the pediatric population performs modestly in detecting hemoperitoneum or intra-abdominal injury, with the following test characteristics: sensitivity of 80% (95% confidence interval [CI] 76% to 84%); specificity of 96% (95% CI 95% to 97%), positive likelihood ratio of 22.9 (95% CI 17.2 to 30.5), and negative likelihood ratio of 0.2 (95% CI 0.16 to 0.25). The high positive likelihood ratio supports prompt cross-sectional imaging of a hemodynamically stable child with suspected abdominal trauma and intraperitoneal fluid seen on FAST. However, a negative ultrasound is not sufficient to definitively rule out the presence of intra-abdominal injury, and therefore, if the pretest probability of injury is high enough, it is reasonable to utilize contrast-enhanced abdominal CT as the initial diagnostic imaging test. Clinicians may consider sonography as the sole diagnostic test in a limited cohort of trauma patients who have a low risk of intra-abdominal injury.
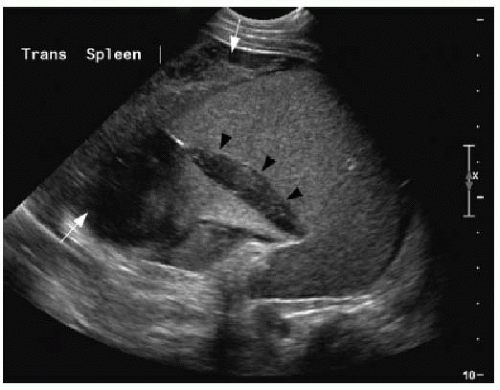
FIG. 18.3 • Focused assessment by sonography for trauma (FAST). Limited abdominal ultrasound performed on a young child presenting in the emergency room after trauma confirms the presence of complex fluid in the left upper quadrant (white arrows) as well as splenic subcapsular hematoma (outlined by black arrowheads).
Only gold members can continue reading. Log In or Register to continue