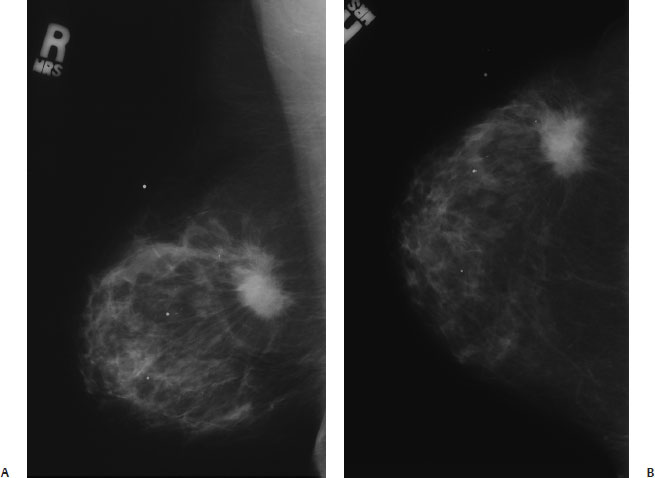
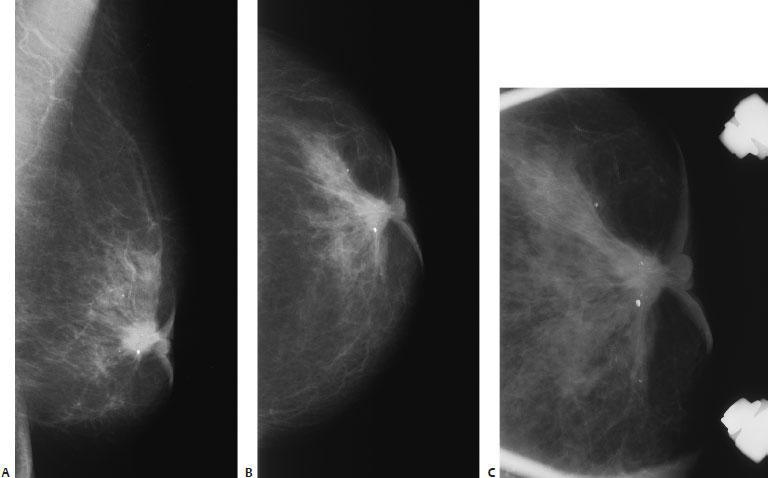
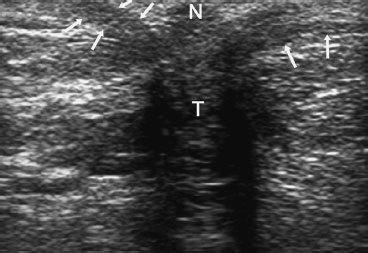
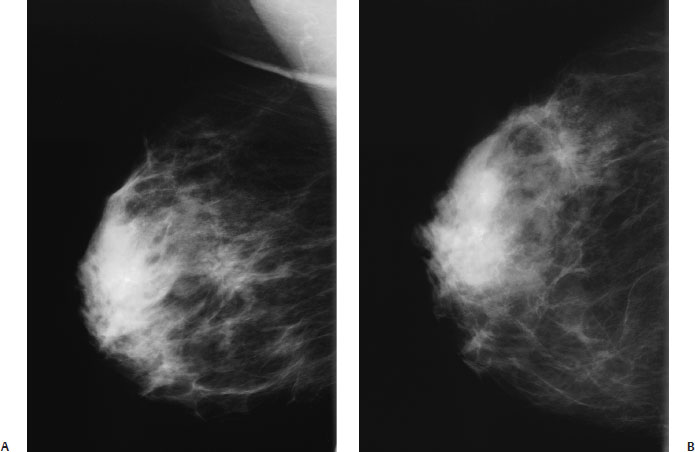
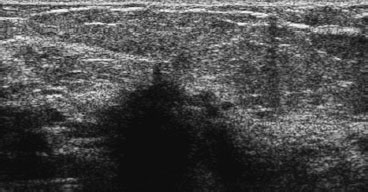
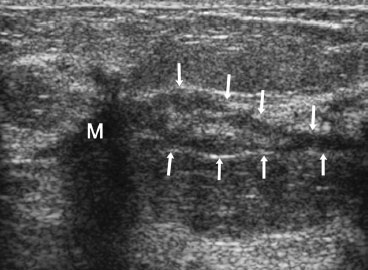
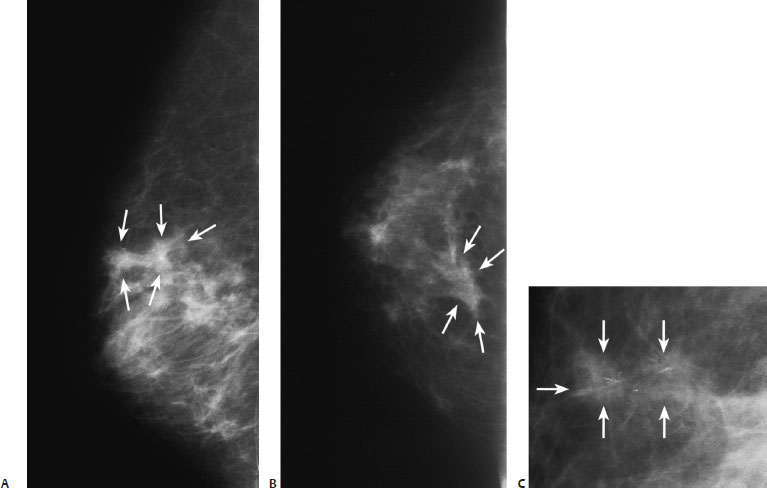
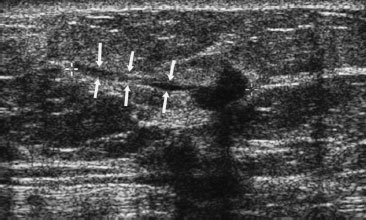
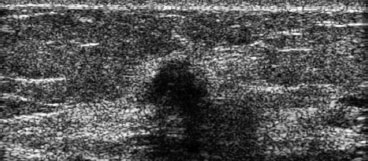
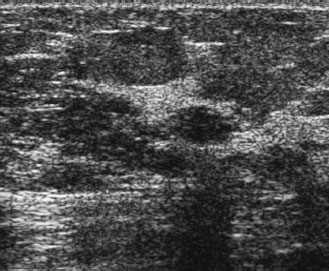
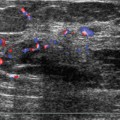
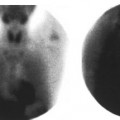
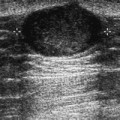
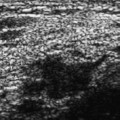
8 Irregular Masses: Malignant Masses A 64-year-old woman presents with back pain, abnormal bone scan, and a right breast lump. • Right breast: palpable lump in the outer breast • Left breast: normal exam Mass (Fig. 8.1) • Margin: spiculated • Shape: irregular • Density: high density Fig. 8.1 In the upper outer quadrant, there is a spiculated mass that corresponds to the patient’s palpable mass. (A) Right MLO mammogram. (B) Right CC mammogram. Other Modalities: Bone Scan (Fig. 8.2) Bone Scan Findings The bone scan demonstrates that the patient’s back pain is due to metastatic disease. Biopsies confirmed that these bone metastases originated from her breast cancer. Fig. 8.2 Technetium-99m whole-body bone scan, posterior view. There are multiple areas of abnormal uptake in the ribs, spine, and right hip consistent with metastatic bony disease. • Infiltrating ductal carcinoma • BI-RADS assessment category 5, highly suggestive of malignancy • Infiltrating ductal carcinoma is the most common breast cancer histology. This cell type represents between 47 and 79% of all invasive breast cancers. The lower percentage has been reported in Japan and the higher percentages in the United States and Scandinavia. • Two thirds of invasive ductal carcinomas appear as irregular mammographic masses. The spiculations consist of a combination of fibrosis and infiltrating tumor. This case illustrates this classic presentation. • In this case, since this mass is highly suggestive of malignancy, and the bone biopsy demonstrated metastatic disease, no biopsy was performed prior to excision. However, if the surgeon wishes to obtain a breast biopsy prior to excision, then one may perform a sonographically guided biopsy may be appropriate as these lesions are generally easily identified with this method. Tabar L, Dean PB. Stellate/spiculated lesions. In: Tabar L, Dean PB. Teaching Atlas of Mammography. 3rd ed. New York: Thieme; 2001:93–147 Tavassoli FA. Infiltrating carcinoma: common and familiar special types. In: Tavassoli FA, Fattaneh A. Pathology of the Breast. 2nd ed. Stamford: Appleton and Lange; 1999:401–480 An 80-year-old woman presents with left nipple retraction. • Left breast: retracted nipple, associated with skin thickening; no definite mass identified • Right breast: normal exam Mass (Fig. 8.3) • Margin: spiculated • Shape: irregular • Density: high density Calcifications • Type: dystrophic • Distribution: grouped/clustered Associated Findings Architectural distortion, skin retraction, skin thickening, trabecular thickening, nipple retraction (Fig. 8.3) Fig. 8.3 There is a spiculated subareolar mass associated with calcifications, skin thickening, and nipple retraction. (A) Left MLO mammo-gram. (B) Left CC mammogram. (C) Left CC spot magnification mammogram. Frequency • 8 MHz Mass (Fig. 8.4) • Margin: spiculation/architectural distortion • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: bilateral edge shadowing • Shape: irregular Fig. 8.4 Left transverse breast sonogram. The sonogram is centered over the nipple (N). Superficially, skin thickening is present (arrows). Deep to the nipple is a solid, irregular, ill-defined, hypoechoic tumor (T). • Invasive ductal carcinoma • BI-RADS assessment category 5, highly suggestive of malignancy • Nipple inversion is due to many etiologies. Benign causes include congenital position, duct ectasia, subareolar abscess, granulomatous mastitis, and postoperative scarring. If the inversion is relatively recent, then carcinoma should be considered. • The mass in this case is highly suggestive of malignancy, so sonography is not needed for characterization of the mass. Sonography was performed for biopsy guidance. Evans AJ, Wilson ARM, Blamey RW, Robertson JFR, Ellis IO, Elston CW. Atlas of Breast Disease Management. Philadelphia: WB Saunders; 1998:32–34 Tavassoli FA, Fattaneh A. Pathology of the Breast, 2nd ed. Stamford: Appleton and Lange; 1999:792–793 A 54-year-old woman presents for screening mammogram. • Normal exam Mass (Fig. 8.5) • Margin: spiculated • Shape: irregular • Density: equal density Fig. 8.5 A spiculated mass is in the right upper outer quadrant. (A) Right MLO mammogram. (B) Right CC mammogram. Frequency • 11.5 MHz • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: severe shadowing, mass completely obscured • Shape: irregular Fig. 8.6 Right radial breast sonogram. The spiculated mass identified in Fig. 8.5 corresponds to an irregular hypoechoic mass with severe acoustic shadowing. Fig. 8.7 Right radial breast sonogram. A few dilated ducts (arrows) extend from the main mass (M) (shown in Fig. 8.6) toward the nipple. The size of the main sonographic mass matches the mammographic size (approximately 2.5 cm). However, if one adds the length of the abnormal ducts, the total length of the abnormality is 5 cm. Only a small portion of the main mass is displayed in this image. Infiltrating ductal carcinoma. The main mass consisted of well-differentiated infiltrating ductal carcinoma. The sono-graphically dilated ducts histologically corresponded to dilated ducts with infiltrating carcinoma within the walls (Fig. 8.8). • BI-RADS assessment category 5, highly suggestive of malignancy Fig. 8.8 Low-power microscopic image of the malignancy demonstrates direct infiltration of tumor cells creating spiculation (arrows). • The breast sonogram suggests that the malignancy is larger than the mammographic density. To confirm this information, sonographically guided biopsies of both the mass and the abnormal ducts were performed. Both the biopsies and the excisional specimen confirmed that the tumor size matched the sonographic size. • Sonographically, dilated ducts that extend from a tumor mass should be viewed as suspicious for additional carcinoma. Tohno D, Cosgrove DO, Sloane JP, eds. Ultrasound Diagnosis of Breast Diseases. New York: Churchill Livingstone; 1994:165–166 A 65-year-old woman has right breast microcalcifications that have been stereotactically mammographically biopsied and are malignant. She now presents for needle localization of these microcalcifications before lumpectomy. • Normal exam Mass (Fig. 8.9) • Margin: indistinct • Shape: irregular • Density: equal density • Calcifications • Type: fine linear/branching • Distribution: grouped/clustered Fig. 8.9 In the upper inner quadrant, there is a cluster of fine linear calcifications. These calcifications are associated with a dumbbell-shaped ill-defined mass (arrows). The shape of this mass and the subtle multinodular pattern of the surrounding parenchyma suggest that the tumor may be multifocal. (A) Right ML mammogram. (B) Right CC mammogram. (C) Right MLO magnification mammogram. Frequency • 10 MHz Mass (Figs. 8.10, 8.11, and 8.12) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: posterior shadowing distal to mass • Shape: irregular Fig. 8.10 Right radial breast sonogram. At the 2 o’clock position, a spiculated mass is associated with the stereotactic biopsy track (arrows). This mass corresponds to the mammographic mass containing the microcalcifications (Fig. 8.9). Fig. 8.11 Right radial breast sonogram. At the 12 o’clock position, a second spiculated solid, mass is present. This mass may be part of the dumbbell structure identified mammographically (Fig. 8.9). Fig. 8.12 Right radial breast sonogram. At the 9 o’clock position there is an oval, ill-defined, solid, shadowing mass. This mass is not mammographically identifiable. Sonographically guided biopsies of this mass and the one in Fig. 8.11 confirmed that they were both malignant. Infiltrating ductal carcinoma. Mastectomy specimen: grossly, the tumor was 4 cm, but random sections outside this mass demonstrated small foci of infiltrating and in situ ductal carcinoma, so the overall size of the malignancy could not be defined. The tumor appeared to be an extensive multifocal malignancy. • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Although the terms multifocal and multicentric appear to be synonymous, they have distinct meanings when applied to malignancy. Multifocality refers to one tumor appearing with multiple closely spaced foci. Multicentricity refers to the simultaneous development of multiple different malignancies. Usually, a tumor is considered multi-focal if the foci are either within the same quadrant of the breast or within 5 cm of each other. • Mammographically, it is important to consider multifocality if there is a suggestion of multiple ill-defined masses closely related to a highly suspicious mass. Sometimes, with multiple oblique magnification views, one can identify spiculations extending from one mass to another. Sonography and an MRI are useful methods to clarify multifocality and guide for biopsy. Berg WA, Gilbreath PL. Multicentric and multifocal cancer: whole-breast US in preoperative evaluation. Radiology 2000;214:59–66 Johnson JE, Dutt PL, Page DL. Extent and multicentricity of in situ and invasive carcinoma. In: Bland KI, Copeland EM, eds. The Breast. Philadelphia: WB Saunders; 1998:296–306 Lagios MD. Multicentricity of breast carcinoma demonstrated by routine correlated serial subgross and radiographic examination. Cancer 1977;40:1726–1734 A 57-year-old woman presents with new right breast dimpling. Mammographically, two suspicious abnormalities are identified: lesion A in the medial inferior breast (which corresponds to the skin dimpling) and lesion B at the 12 o’clock position. Unfortunately, only the 12 o’clock position mass (B) is adequately localized for biopsy. The medial inferior abnormality (A) is not confidently identified during an attempt to perform mammographic stereotactic biopsy and is not localized on the initial breast sonogram. Lesion A is identified only sonographically after breast MRI demonstrates the mass. • Right breast: subtle skin dimpling in medial breast associated with vague firmness • Left breast: normal exam Mass (Fig. 8.13) • Margin: indistinct • Shape: irregular
Case 8.1: Infiltrating Ductal Carcinoma
Case History
Physical Examination
Mammogram

Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 8.2: Infiltrating Ductal Carcinoma
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 8.3: Infiltrating Ductal Carcinoma
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management

Pearls and Pitfalls
Suggested Reading
Case 8.4: Infiltrating Ductal Carcinoma
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 8.5: Infiltrating Ductal Carcinoma
Case History
Physical Examination
Mammogram
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


