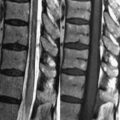
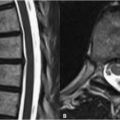
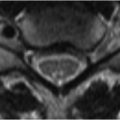
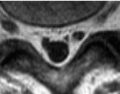
14 Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the anterior choroidal artery of the supraclinoid portion of the ICA, the lenticulostriate branches of the ACA and MCA, the thalamoperforating branches of the posterior cerebral arteries (PCA), and the paramedian branches of the basilar artery. These infarcts are associated with chronic hypertension and may present clinically with pure motor or sensory deficits. On MRI lacunar infarcts appear as focal slitlike or ovoid areas, progressing in appearance similarly to the infarcts described in Chapter 13. The lenticulostriate branches of the MCA originate prior to the artery’s bi- or trifurcation (M1 segment) to supply the basal ganglia and the anterior limb of the internal capsule. Thus ischemic disease involving the MCA prior the branching of the lenticulostriate arteries may involve its hemispheric distribution along with deep gray and white matter structures. A similar phenomenon is seen with the thalamoperforating arteries of the PCA. Figure 14.1A demonstrates acute ischemia of the lentiform nucleus, which consists of the globus pallidus (medially) and the putamen (laterally), shown on a DWI scan. Note that the susceptibility effects of iron within the globus pallidus result in this structure’s low SI on T2WI (such as DWI) at 3 T (Fig. 14.1A). Figure 14.1B demonstrates in the same patient an acute infarction of the head of the caudate as seen on DWI. The head of the caudate is supplied by the recurrent artery of Heubner, which arises from the ACA to also supply the anterior limb of the internal capsule and part of the putamen. The anterior choroidal artery, arising from the supraclinoid internal carotid, also supplies portions of the caudate, along with the posterior limb of the internal capsule and parts of the thalamus, globus pallidus, and cerebral peduncles. DWI is particularly useful in the evaluation of lacunar strokes, due to the tendency of chronic small vessel ischemia to obscure the appearance of high SI infarcts on FLAIR (Fig. 14.1C) and T2WI. Such lesions are clearly differentiated from chronic ischemic changes on DWI (Fig. 14.1B). Lesions of multiple sclerosis (see Chapter 18), Binswanger disease (a triad of hypertension, hydrocephalus, and dementia), and hypertensive encephalopathy are similarly easily distinguished from acute and early subacute lacunar infarcts. The thalamoperforating arteries arise from the P1 segment of the PCA. These supply the medial ventral thalamus and the posterior limb of the internal capsule. An infarction of this region, as seen on DWI, is denoted by a white arrow
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


