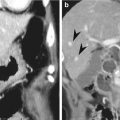
Fig. 12.1
Small bowel infarction due to SMA embolism. Axial contrast-enhanced CT shows nonenhancing SMA due to embolism (arrow). Small bowel loops are dilated filled with fluid and the walls show no enhancement (white arrowheads). Also note ascites (black arrowheads). Asterisks indicate intraluminal air in the infarcted small bowel loops
12.3.2 Small Bowel Infarction
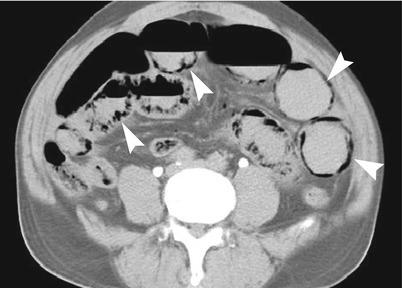
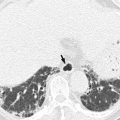
Fig. 12.2
Small bowel infarction. Axial contrast-enhanced CT shows intramural air bubbles of small bowel, pneumatosis intestinalis, as well as no enhancement of the small bowel wall (arrowheads)
12.3.3 Small Bowel Infarction
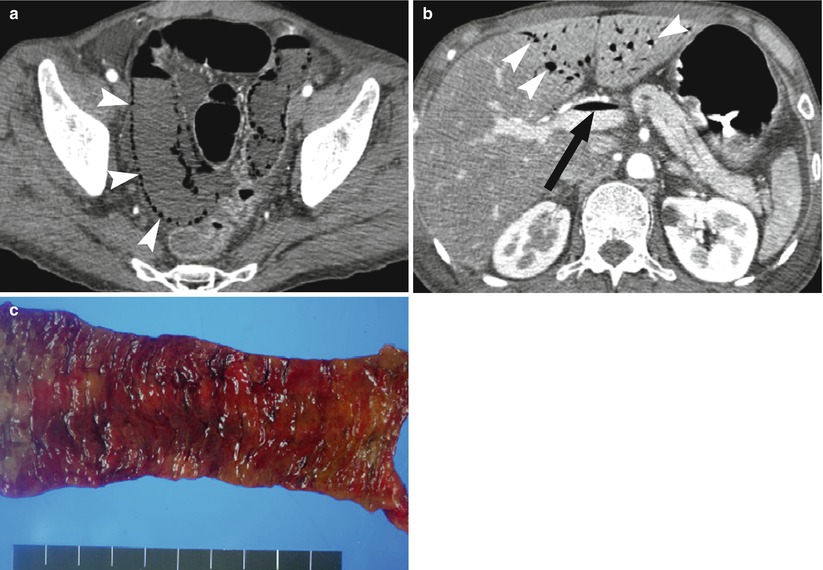
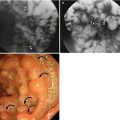
Fig. 12.3
Small bowel infarction. (a) Axial contrast-enhanced axial CT scan reveals pneumatosis intestinalis of the small bowel and absence of bowel wall enhancement (arrowheads). (b) Air in the main portal vein (arrow) and intrahepatic portal vein branches (arrowheads) is another sign of severe mesenteric ischemia. (c) Resected small bowel specimen shows diffuse mucosal infarction
12.3.4 SMA Embolism in a 64-Year-Old Man
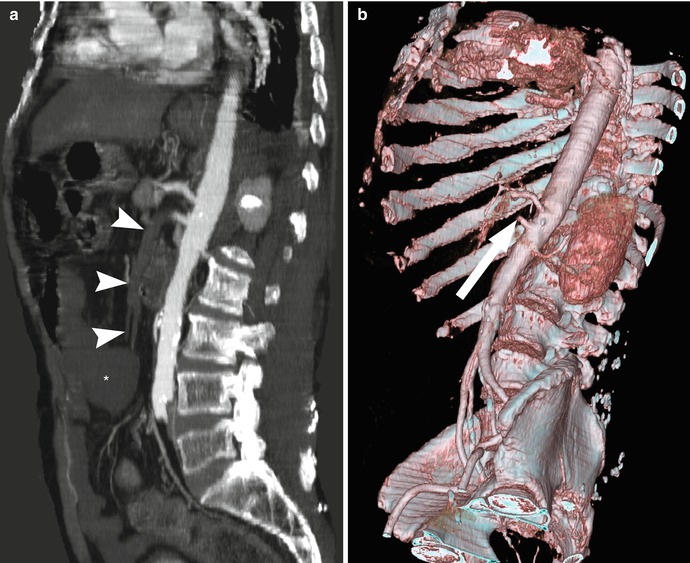
Fig. 12.4
SMA embolism in a 64-year-old man with atrial fibrillation who presented with acute abdominal pain. (a) Sagittal contrast-enhanced CT shows filling defect of SMA (arrowheads) and small bowel lacking wall enhancement (asterisk), suggesting infarction due to SMA embolism. (b) Volume-rendered image of the CT scan shows abrupt cutoff of SMA (arrow) due to embolism
12.3.5 SMA Dissection and Thrombosis in a 49-Year-Old Man
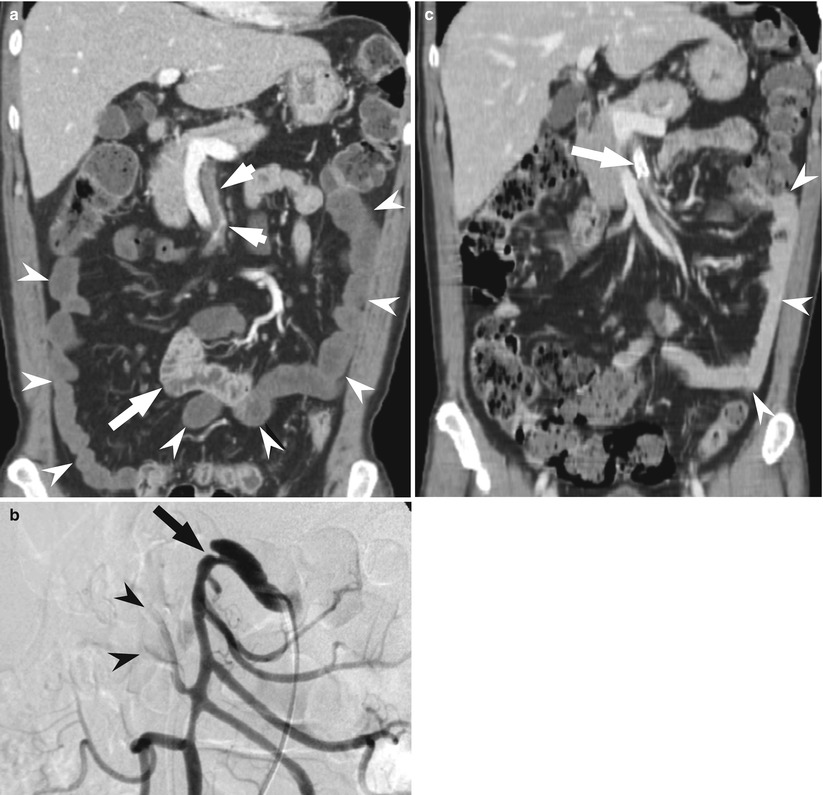
Fig. 12.5
SMA dissection and thrombosis in a 49-year-old man who presented with abrupt periumbilical pain. (a) Coronal image of enhanced CT scan shows thrombosis in the SMA (short arrows). Note ischemic small bowel loops showing no wall enhancement (arrowheads) in contrast to viable bowel segment showing wall enhancement (long arrow). (b) SMA angiography shows proximal SMA dissection (arrow) with diminished flow of jejunal branches (arrowheads). (c) After stent placement at the dissected segment of SMA (arrow), distal arterial flow is preserved and small bowel viability is restored (arrowheads)
12.3.6 SMV Thrombosis
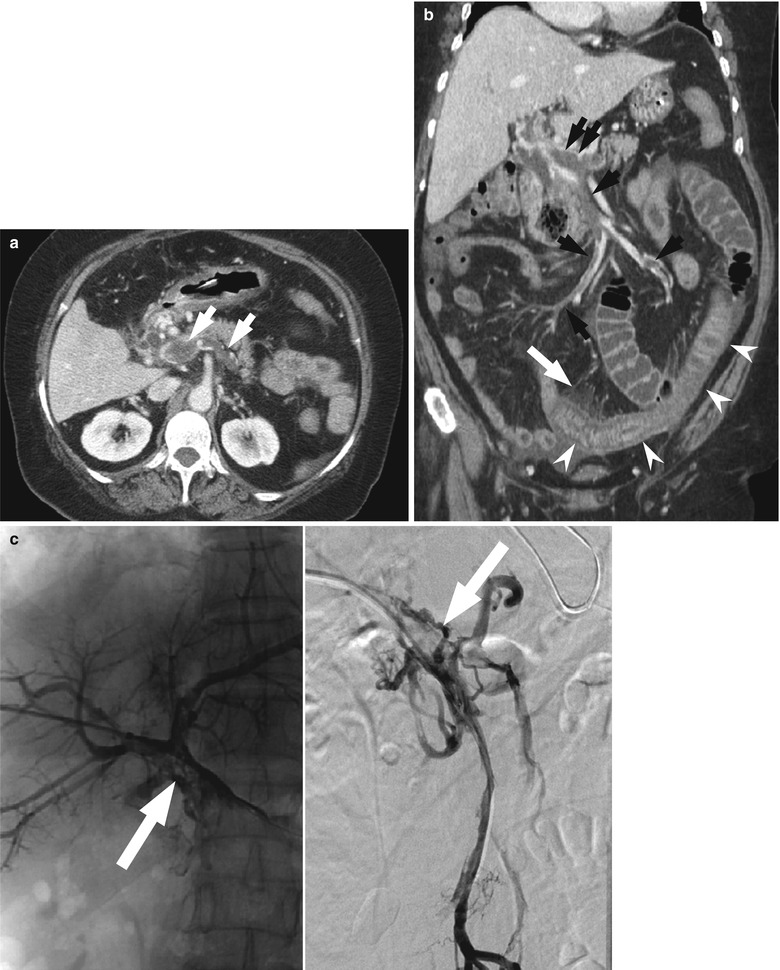
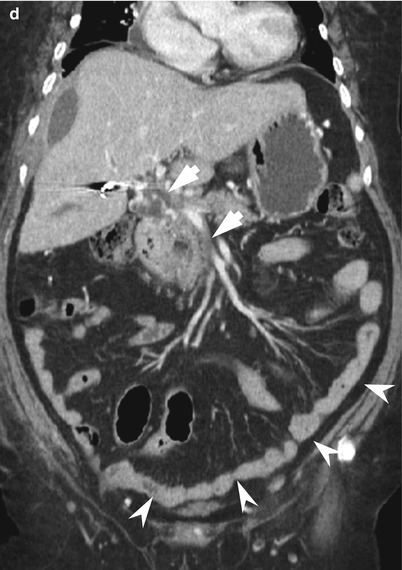
Fig. 12.6
SMV thrombosis. (a) Enhanced CT shows filling defect in the SMV and splenic vein (arrows), suggestive of thrombosis. (b) Coronal image shows multifocal thrombosis in the main portal vein, SMV, and its jejunal branches (black arrows). Affected small bowel segment shows wall thickening with mucosal enhancement and submucosal edema (white arrowheads), as well as mesenteric fat stranding (white arrow). (c) Percutaneous transhepatic portography shows thrombosis in the main portal vein (left) and SMV (right). Overnight thrombolysis was performed. (d) Coronal image of follow-up CT a week after thrombolysis shows decreased extent of portomesenteric venous thrombosis (arrows) and normalized small bowel loops (arrowheads)
12.3.7 Idiopathic SMV Thrombosis
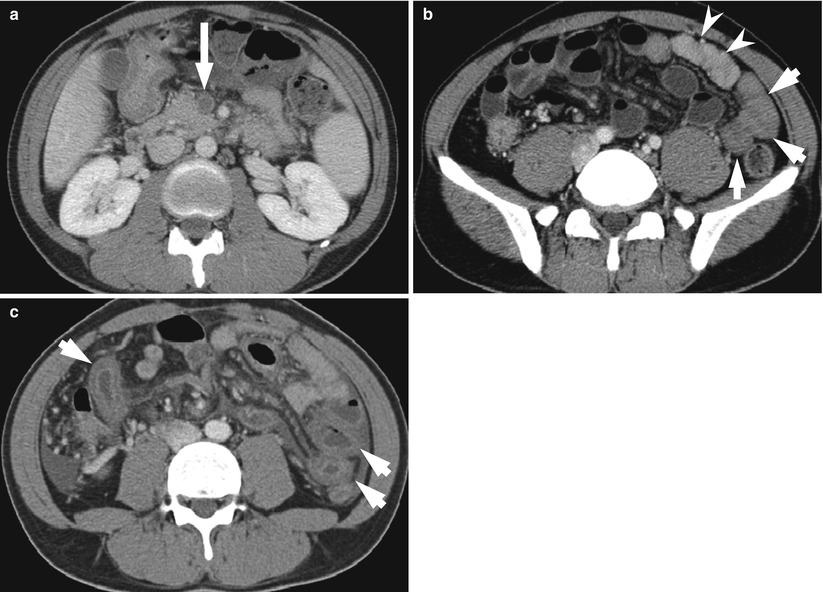
Fig. 12.7
Idiopathic SMV thrombosis. (a) Axial contrast-enhanced CT shows SMV thrombosis (arrow). (b) Note the ischemic small bowel segments with decreased enhancement (arrows), compared with neighboring normal bowel loops (arrowheads). (c) Follow-up CT two days later shows progressed small bowel thickening with target appearance (arrows) and ascites
12.3.8 Idiopathic SMV Thrombosis in a 39-Year-Old Man
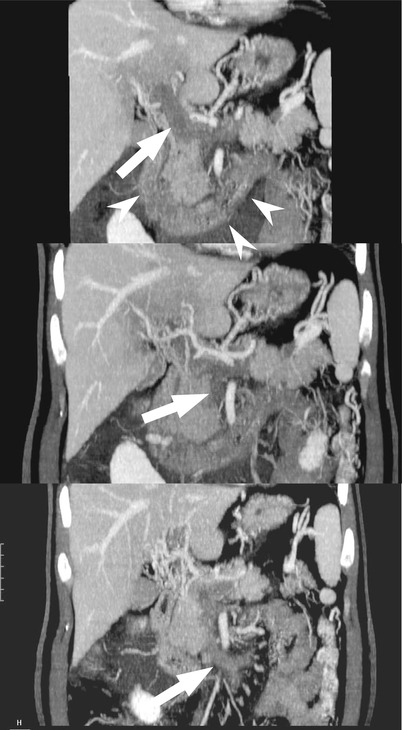
Fig. 12.8
Idiopathic venous thrombosis in a 39-year-old man who presented with right upper quadrant pain for 2 weeks. MIP (maximum-intensity projection) images of contrast-enhanced CT show thrombosis in the main portal vein, SMV, and IMV (white arrows from top to bottom). Also note edematous thickening of duodenum (arrowheads)
12.3.9 SMV Thrombosis in a 65-Year-Old Woman
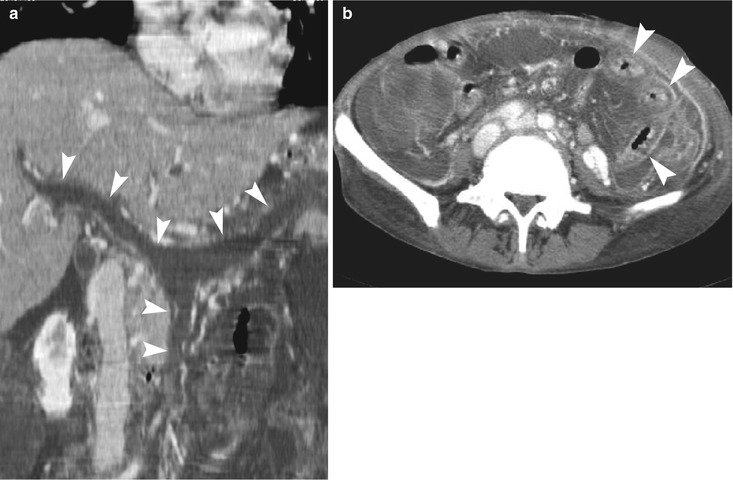
Fig. 12.9
SMV thrombosis in a 65-year-old woman who had polycythemia vera and underwent splenectomy. (a) Curved multiplanar reformatted image shows whole thrombosis in the portal vein, splenic vein, and SMV (arrowheads). (b) Axial CT image shows edematous thickening of the small bowel loops (arrowheads). Resected small bowel specimen revealed ischemic infarction due to thrombotic microangiopathy
12.3.10 Hemorrhagic Infarction of the Small Bowel
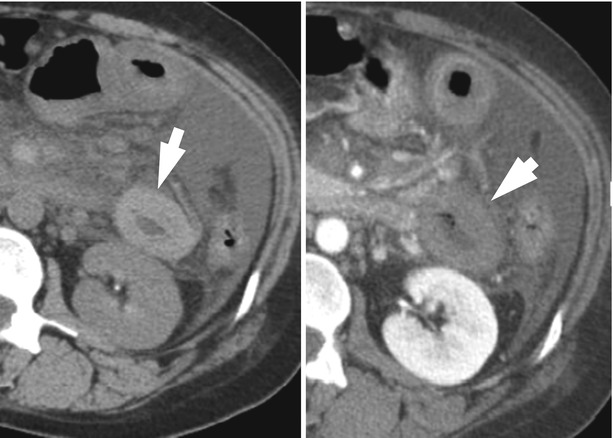
Fig. 12.10
Hemorrhagic infarction of the small bowel. Axial nonenhanced CT (left) shows high density of the small bowel (arrow) that lacks enhancement on corresponding enhanced CT (right, arrow), suggesting hemorrhagic infarction
12.3.11 Closed-Loop Obstruction and Hemorrhagic Infarction of the Small Bowel
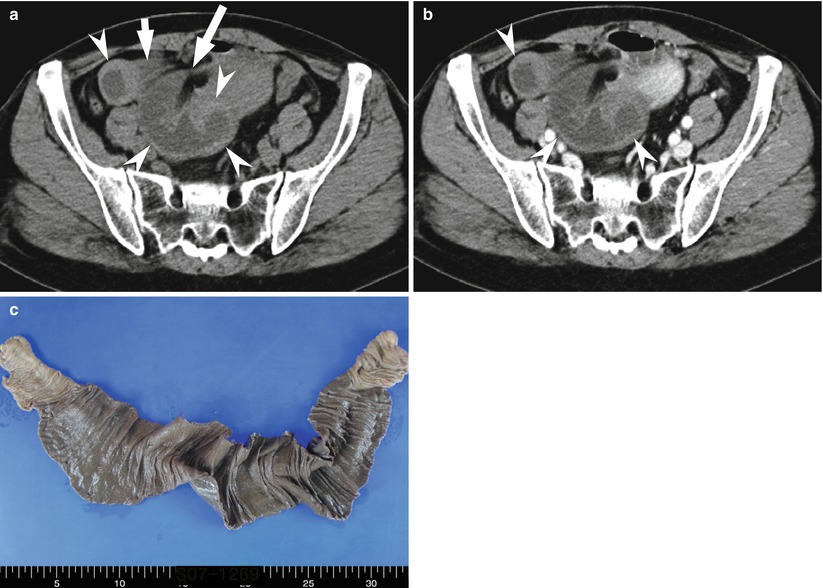
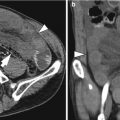
Fig. 12.11
Closed-loop obstruction and hemorrhagic infarction of the small bowel in a 47-year-old woman. (a) Unenhanced CT image shows high-density thickening (arrowheads) with beak appearance (long arrow) of the small bowel loops and mesenteric stranding (short arrow). (b) Enhanced image shows no significant wall enhancement of the corresponding small bowel (arrowheads), suggestive of hemorrhagic infarction. (c) Resected small bowel segment shows hemorrhagic infarction
12.3.12 Small Bowel Infarction Due to Strangulating Obstruction
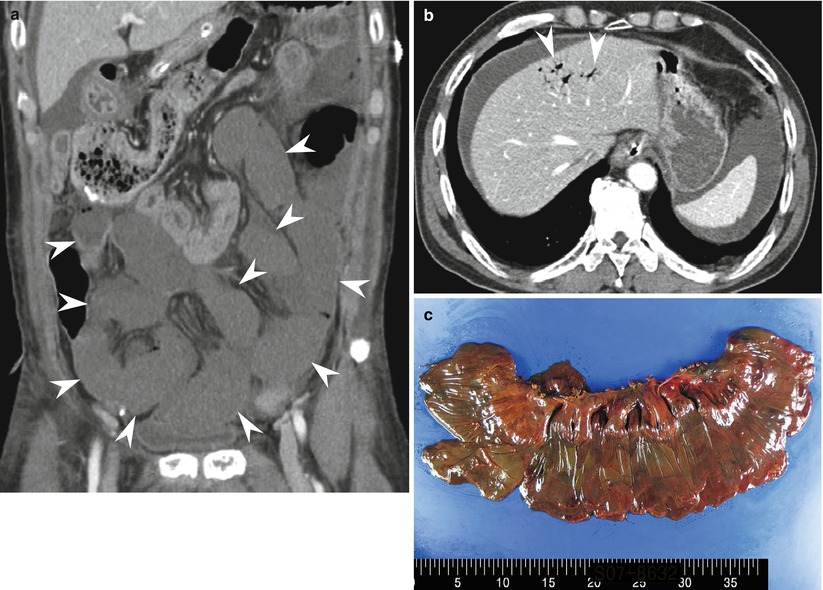
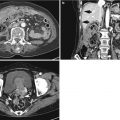
Fig. 12.12




Small bowel infarction due to strangulating obstruction. (a) Coronal contrast-enhanced CT shows long segmental dilatation and lack of wall enhancement of the small bowel (arrowheads) suggesting bowel infarction. (b) Axial contrast-enhanced CT shows air in the portal vein branches (arrowheads) and ascites. (c) Resected small bowel demonstrated hemorrhagic infarction due to band formation and strangulation
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
