Chapter 77 Juvenile angiofibroma (JNA) accounts for < 0.5% of head and neck neoplasms. These benign but locally aggressive tumors are found almost exclusively in adolescent males. It is believed that the lesion originates in the region of the sphenopalatine foramen at the junction between the posterior nasal fossa and the nasopharynx. The vast majority of patients are diagnosed relatively late in the course of the disease. Symptoms are usually present for at least 6 to 12 months before diagnosis. Nasal obstruction is the most common symptom followed by epistaxis. Other signs and symptoms include facial swelling, proptosis, and visual disturbance such as diplopia. These lesions are well circumscribed and appear deceptively avascular on clinical inspection. The tumor consists of a fibrous stroma of spindle-shaped cells and a rich network of irregular vascular channels. These vascular channels are lined by endothelium but they lack surrounding smooth muscle support. This phenomenon appears to contribute to the capacity for massive hemorrhage following manipulation. The most widely accepted treatment is embolization followed by resection. Very advanced lesions that have aggressive skull base erosion may be treated with radiation therapy. Residual tumor may regress after puberty because the growth of the tumor is felt to be hormonally based. These are characteristically hypervascular tumors. The classic tumor is centered in the sphenopalatine foramen and widens this foramen. The tumors extend laterally into the pterygopalatine fossa and widen the fossa. The posterior wall is often thinned and displaced anteriorly. Continued spread through the pterygopalatine fossa may result in extension into the masticator space or may follow the infraorbital fissure into the orbital apex. Medial spread from the sphenopalatine foramen will result in extension into the posterior nasal cavity and nasopharynx. Advanced disease may result in intracranial extension via the superior orbital fissure or aggressive skull base erosion. Occasionally, JNA may be primarily centered in the posterior nasal cavity and nasopharynx without significant extension into the pterygopalatine fossa (Figs. 77–1, 77–2, and 77–4
Juvenile Angiofibroma
Epidemiology
Clinical Findings
Pathology
Treatment
Imaging Findings
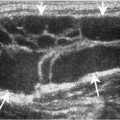
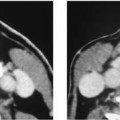
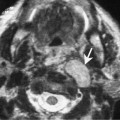
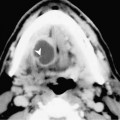
CT
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


