Chapter Outline
Introduction
Ultrasound has an important role to play in the investigation of pathology relating to the knee. However, it is important to recognize it has significant limitations, particularly with regard to the demonstration of intraarticular pathology involving structures such as the menisci, cruciate ligaments and articular cartilage. Consequently ultrasound is predominantly used for the assessment of extraarticular pathology about the knee and is particularly useful for diagnosing conditions affecting the tendons, muscles, ligaments, bursae and soft tissues. Dynamic assessment, comparison with the contralateral side and the ability to undertake sonopalpation (the displacement or movement of structures with probe pressure) are all valuable advantages of ultrasound over other modalities.
Tendons
Patellar Tendon
The patellar tendon is a relatively superficial structure readily examined by ultrasound. Patellar tendinopathy is a condition commonly caused by overuse, particularly as a result of running and jumping activities; it has been also termed ‘jumper’s knee’ and is thought to result from chronic microtrauma to the tendon. Patients usually present with anterior knee pain that is most frequently localized over the lower pole of the patella. Appearances on ultrasound are of disruption of the normal fibrillar pattern and thickening of the tendon with focal areas of hypoechoic change within it, associated with neovascularity within the tendon as a result of vascular in-growth ( Fig. 22.1 ).
Changes of patellar tendinopathy are usually focal, most commonly affecting the deeper fibres of the proximal tendon either centrally or towards the medial side of the tendon.
| Neovascularization is best demonstrated on power Doppler imaging with the knee extended and with only light probe pressure over the tendon. |
| Tendinopathy involving the entire tendon is not usually related to physical activity but to systemic disorders leading to infiltration of the tendon, such as gout and hypercholesterolaemia ( Fig. 22.2 ). |


Rupture of the patellar tendon may occur, resulting in a complete disruption of the extensor mechanism. This most frequently occurs on a background of preexisting tendinopathic change or in the presence of systemic inflammatory conditions such as diabetes, rheumatoid arthritis, systemic lupus erythematosus (SLF) or chronic renal failure. Both systemic steroids and local steroid injections have also been shown to be contributing factors. Following rupture, a high-riding patella may be detected on clinical examination or conventional radiography as a result of retraction by the quadriceps mechanism ( Fig. 22.3 ). On ultrasound, patella alta results in the trochlear groove, normally hidden behind the patella, becomes visible, while examination of the tendon itself will demonstrate the discontinuity ( Fig. 22.4 ). Interposed haematoma may make visualization of the tendon ends difficult; however, dynamic assessment of the tendon should allow differentiation of partial- from full-thickness injury.


Acute avulsion injuries involving the patellar tendon are rare in adults and often occur secondary to high-impact trauma or eccentric muscle contraction. In the paediatric population this injury is termed a patellar sleeve fracture; in this condition a sleeve of cartilage is pulled off the main bony patella, often taking with it a small bony fragment from the lower pole.
Osgood–Schlatter’s Disease
Chronic inflammation of the insertion of the patellar tendon onto the tibial tuberosity may be seen in adolescents ( Fig. 22.5 ). This condition, called Osgood–Schlatter’s disease, represents a traction enthesopathy and is characterized by irregularity of the tibial tuberosity. The tibial tuberosity may be irregular in asymptomatic patients and care should be taken to avoid overdiagnosing this condition. Reactive secondary heterotopic bone formation occurs at the insertion site of the patellar tendon, resulting in a visible and palpable lump: the main physical finding in Osgood–Schlatter’s disease. A similar condition occurring at the patellar insertion is termed Sindig-Larsen–Johansson syndrome. On ultrasound, thickening of the patellar tendon at the insertion site with low-reflective change and associated intratendinous calcification is seen ( Fig. 22.6 ). Neovascularization may also be present in the tendon and peritendinous bursitis may also be shown. Ultrasound will also demonstrate bony surface irregularity and/or fragmentation of the tibial tuberosity (Osgood–Schlatter’s disease) or lower pole of the patella (Sindig-Larsen–Johansson syndrome).


Quadriceps Tendon
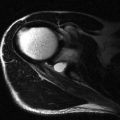
The quadriceps tendon is less commonly affected by tendinopathic change than the patellar tendon and when seen it usually relates to persistent strenuous overuse. Clinically the condition presents as focal pain over the distal portion of the tendon and will manifest on ultrasound as a focal area of hypoechoic change within a portion of the tendon, loss of definition of the normal trilaminar appearance and intratendinous vascularity. Transverse imaging of the tendon is often helpful in more accurately defining the precise location of the tendinopathic change. More rarely the full thickness of the tendon is involved and appearances will be of diffuse thickening of the tendon with heterogeneous echotexture throughout ( Fig. 22.7 ).

Rupture of the quadriceps tendon is a relatively rare phenomenon.
The majority of tears are incomplete and involve only one of the tendon components: most commonly the tendon component arising from rectus femoris.
| The squeeze test involves lateral compression of the joint in an attempt to force joint fluid into the prepatellar space. This can only occur in the presence of a full-thickness defect. |

Other Tendons
Other tendons around the knee may also become tendinopathic and may rarely rupture. Most commonly involved is the semimembranosus tendon which presents with pain in the posteromedial aspect of the joint. The insertion of this tendon is difficult to visualize on ultrasound due to its depth and MRI may be more helpful in delineating pathology here. Tendinopathy of the distal biceps femoris, semitendinosus ( Fig. 22.9 ), gracilis and sartorius also occur. Distal biceps femoris rupture most often occurs in conjunction with lateral collateral ligament disruption, often in association with an anterior cruciate ligament (ACL) tear of the knee.

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


