• Understand the normal imaging anatomy of the larynx and hypopharynx particularly in context of the clinical setting.
• Review updated scanning techniques and understand the embryology and anatomy-based imaging issues.
• Read the larynx and hypopharynx imaging studies according to standard anatomical levels and identify subsite-specific structures at each of these levels.
• Approach to interpreting and reporting laryngeal and hypopharyngeal SCCa. Updated TNM staging.
• Posttreatment imaging of the larynx and hypopharynx.
• Nonepithelial tumours and tumour mimics.
• Nonneoplastic conditions of larynx and hypopharynx (infections, inflammations, vocal cord paralysis, laryngoceles and trauma).
Introduction
The larynx is a mucosa lined tube supported by a cartilaginous and muscular framework ably supported by multiple ligamentous and membranous structures. It acts as a critical connection between the oropharynx above and the trachea below serving essential functions such as respiration, phonation and preventing aspiration.
The hypopharynx is a small but critical component of the pharynx situated posterior to the larynx with a similar craniocaudal extent connecting the oropharynx above to the cervical oesophagus below.
As these structures are close to each other, the anatomical and pathological features are always described concomitantly. However, it must be clearly understood, as a basic concept, that the larynx and the hypopharynx are two completely different anatomic entities with separate subsites, pathologies and management protocols.
Embryology
The larynx develops from the fourth to the sixth branchial arches. Each of the arches contains a core of mesenchymal tissue (from the lateral and paraxial mesoderm). The core of the fourth branchial arch forms the extrinsic musculature, including the cricothyroid muscle, levator veli palatini and the pharyngeal constrictors. These structures are supplied by the superior laryngeal branch of the vagus nerve. The core of the sixth branchial arch forms the intrinsic laryngeal musculature supplied by the recurrent laryngeal branch of the vagus nerve. Cores of all branchial arches (fourth to sixth) also receive migrating neural crest cells that form the skeletal components of the larynx, i.e., thyroid, cricoid, corniculate and cuneiform cartilages.
Embryological development of the endolarynx from different structures determines the lymphatic drainage and hence the clinical presentation of laryngeal cancers. An imaginary line drawn through the laryngeal ventricle just above the glottis defines the two embryologically separate parts of the larynx, which determine the lymphatic drainage pathways. The supraglottis develops from the buccopharyngeal anlage; the glottis and the subglottis derive from the tracheobronchial buds.
Imaging modalities, protocols and special techniques
Irrespective of the modality that is being used, it is essential to ensure an optimal study. This can be achieved by the following:
• Explaining the procedure to patient.
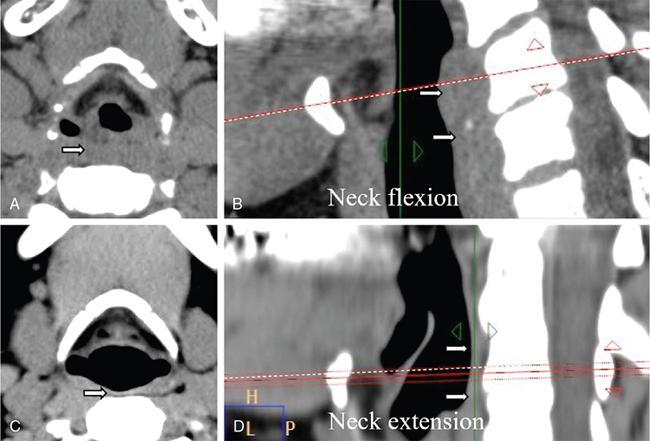
• Conducting the study in a comfortable supine position with neck slightly extended. This prevents artifactual thickening of the posterior laryngopharyngeal soft tissues and also minimizes swallowing artefacts (Fig. 3.11.1).
• Issuing repeated instructions to the patient: continue quiet nasal respiration; avoid swallowing/coughing and moving the neck.
• Optimizing intravenous contrast administration with regards to concentration, volume and scan delay. 100 mL of 400 mgI/mL nonionic intravenous contrast medium with a saline chaser at an infusion rate of 3 mL/s after a 70-second delay is recommended for optimal visualization of the pathology, internal characteristics of the lesion and differentiating the lesion margins from surrounding healthy tissue. Contrast medium of similar strength is administered to the pediatric population in a dose of 2 ml/kg body weight (not exceeding a total dosage of 40 ml).
• Performing breath-manoeuvre laryngeal computed tomography (BML CT) with images obtained in breath-hold and during phonation/Valsalva.
• Performing magnetic resonance imaging (MRI) using dual phased array surface coils and customized protocols
• Reviewing and modifying sequences whilst the scan is being conducted.
Fig. 3.11.1Larynx CT – effect of neck flexion on image interpretation. Axial/reconstructed sagittal CT images at the level of the hyoid bone. Images with neck flexion (A,B) show artifactual thickening of posterior pharyngeal wall ( arrows) which resolves to normal thickness ( arrows) in images obtained with mild neck extension (C,D). Mild extension of neck also minimizes swallowing artefacts.
CT
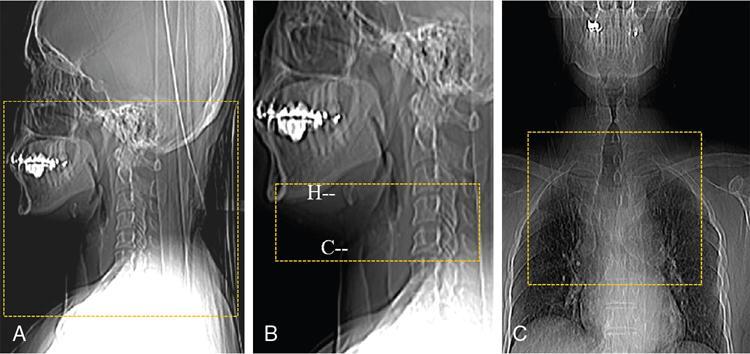
In many centres across the world, contrast-enhanced multidetector CT (MDCT) is the preferred modality of choice using a two-pass technique and customized field of view (Fig. 3.11.2). The first contrast-enhanced pass is performed from the hard palate to the clavicle in quiet respiration, and the second limited pass is performed from the hyoid bone to the inferior aspect of the cricoid cartilage in Valsalva/phonation and breath-hold (Fig. 3.11.3). An extended study may be conducted if necessary, to assess the upper chest till the level of the pulmonary hilum (Fig. 3.11.2C). Overlapping sections must be obtained for optimal multiplanar reconstructions (0.67 mms reconstruction slice thickness with 0.33 mms reconstruction interval is recommended in areas of interest). MDCT is readily available, is a fast scanning technique and covers a large field of view. It also evaluates the lung fields at the same sitting. However, it is fraught with misdiagnosis and interpretive errors concerning early cartilage invasion by tumour tissue.
Fig. 3.11.2Larynx CT scan range: Precontrast and first-pass postcontrast scan (A), breath-manoeuvre scan from hyoid (H) to cricoid (C) (B) and extended upper thorax scan (C).
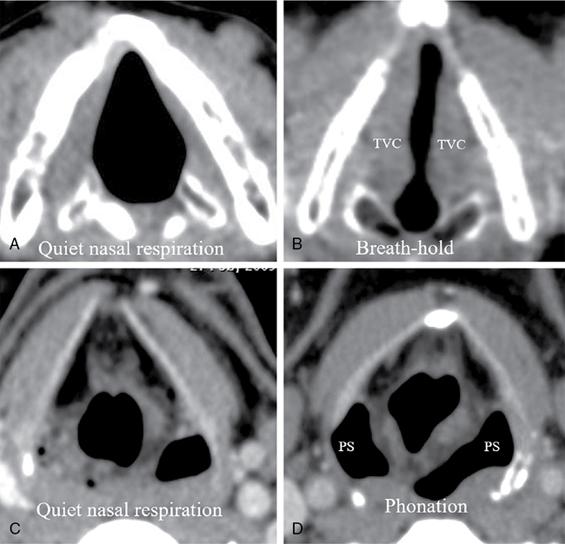
Fig. 3.11.3Breath-manoeuvre Larynx CT. Axial CT images at the level of the true vocal cords (TVCs) in quiet nasal respiration and in breath-manoeuvre (A,B). Axial CT images at the level of the piriform sinuses (PS) in quiet nasal respiration and in phonation manoeuvre (C, D).
MRI
In many centres, MRI is the preferred modality to image of the larynx and hypopharynx. It has distinctive advantages if performed using high-field MR (minimum 1.5 Tesla), dual phased array surface coils (Fig. 3.11.4) in combination with the neurovascular coil and specially customized protocols. Patient cooperation and compliance is also an important prerequisite to obtaining optimal diagnostic quality MRI images in this region.
Fig. 3.11.4Larynx MRI – use of dual phased array surface coils for increasing resolution of laryngeal structures.
Advantages of MRI:
1. High resolution depicting excellent anatomical detail (Fig. 3.11.5).
2. Better evaluation of local tumour and cartilage invasion for accurate T and N staging. The local tumour extension is better visualized (especially glottic T1 and T2 stages). It also evaluates deep invasion of the true vocal cords (helps in deciding if the lesion can be treated by laser therapy).
3. Better soft tissue definition of the preepiglottic/paraglottic fat spaces, anterior commissure and extralaryngeal spread.
4. Better craniocaudal extension evaluation of the lesion in cases with subglottic extension, thyrohyoid membrane and cartilage edge involvement.
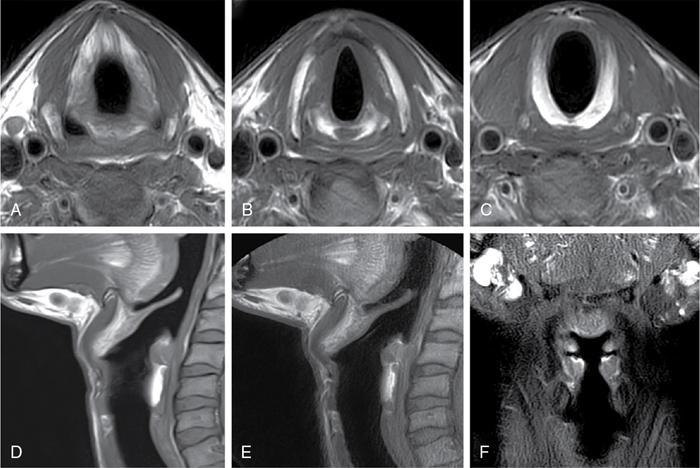
Fig. 3.11.5Larynx MRI – surface coil imaging. T1W axial images at supraglottic (A), glottic (B) and subglottic (C) levels. T1W sagittal (D) and STIR sagittal (E) and coronal (F) images.
Disadvantages of MRI:
1. More susceptible to motion, swallowing and breathing artefacts
2. A suboptimally performed study results in low-resolution images, decreased signal-to-noise ratio and longer examination times
3. Reduced availability of advanced MRI scanners/coils in developing and underdeveloped countries.
FDG PET-CT
• Pretreatment: for staging locally advanced disease, to assess nodal status (unilateral/bilateral/clinically inaccessible nodes in the retropharyngeal space, visceral space and chest), to identify the presence of the unknown primary neoplasm (which may be in endoscopically occult locations like the pyriform sinuses and upper subglottic region) and to detect distant metastases.
• Posttreatment: as a baseline investigation (performed 12 weeks after the completion of therapy), to differentiate residual/recurrent tumour from posttreatment changes and restaging in recurrent disease/nodal and distant metastatic disease.
Ultrasonography
USG, with the present-day high-frequency, high-resolution transducers, is useful not only in benign laryngeal pathologies (Reinke space oedema, vocal nodules, polyps and cysts) but also in staging locally restricted malignancies, assessing vocal cord mobility and in posttreatment surveillance.
It is readily available, noninvasive, does not involve ionizing radiation and can be performed in uncooperative patients who have difficulty breathing and are coughing. US also has the added advantage of evaluating nodal status (pre- and posttreatment) and can be combined with US-guided fine-needle aspiration (FNA) or biopsy.
TEACHING POINTS BOX 1:
• The buccopharyngeal anlage/supraglottis contains an abundant lymphatic network that drains into the upper deep cervical nodal chain, and hence, cancers arising from this region often present with lymph node metastasis. The tracheobronchial buds/glottis and subglottis contains fewer lymphatic channels and is relatively avascular, so the tumours confined to these structures generally do not metastasize into the regional lymph nodes. These cancers drain to the low deep cervical nodal chain and the paratracheal nodal chain if they do. These tumours, therefore, do not present with metastatic nodes but with related symptoms, i.e., change of voice, hoarseness of voice and difficulty in breathing.
• The respiratory phase alters laryngeal and hypopharyngeal anatomy during scan acquisition which may affect the imaging appearance of the anatomical structures and result in an asymmetric appearance of the aryepiglottic folds/pyriform sinuses. This should not be mis-interpreted as an abnormal finding. The two-pass technique allows comparison of structures which may have changing appearances due to different respiratory phases.
Anatomy
The hypopharynx and larynx share the identical cranio-caudal extent. The larynx is situated anterior to the hypopharynx and both structures have distinctly separate anatomical subsites (Fig. 3.11.6).
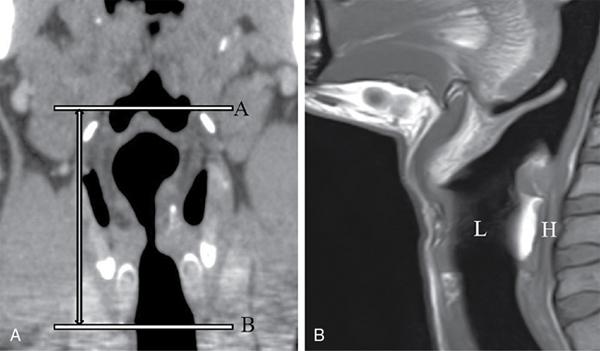
Fig. 3.11.6Coronal CT image (A) shows identical cranio-caudal extent of the larynx and hypopharynx from the level of the glosso-epiglottic and lateral pharyngoepiglottic folds ( Line A) till the lower margin of the cricoid cartilage ( Line B). Sagittal TIW image shows anterior larynx (L) and posterior hypopharynx (H).
Hypopharynx
The hypopharynx is a crucial component of the upper aero-digestive tract (more of the digestive tract than the airway), connecting the oropharyngeal mucosal space to the oesophagus and is located posterior to the larynx. At its superior limit, the hyoid bone, the glosso-epiglottic fold and the pharyngoepiglottic fold demarcate the vallecula, which are part of the oropharynx. The cricopharyngeus muscle defines the inferior limit of the hypopharynx, just below the cricoid cartilage. The hypopharynx is a mucosal and muscular tube with five distinctive layers: mucosa (stratified squamous epithelium), submucosa (loose stromal tissue with fat), fibrous layer (inferior continuation of the pharyngo-basilar fascia), muscular layer (middle and inferior constrictors) and the fascial layer (continuation of the middle layer of the deep cervical facia).
Larynx
The larynx extends superiorly from the level of the median glosso-epiglottic fold and lateral pharyngo-epiglottic folds (generally considered at the level of the hyoid bone) till the undersurface of the cricoid cartilage inferiorly.
It is practical to classify the larynx as:
a. Exolarynx: consisting of the cartilages, muscles, ligaments and membranes surrounding and supporting the larynx.
b. Endolarynx: the mucosal surfaces adjacent to the airway and the submucosal soft tissues. The endolarynx is classified into three subsites: supraglottis, glottis and subglottis (discussed under imaging anatomy subsites).
The exolarynx
As the hyoid bone is an important landmark, it is pertinent to start the discussion with this U-shaped bone located in the midline anterior upper neck. It is attached to the upper edge of the thyroid cartilage by the thyrohyoid membrane, thus reinforcing the upper larynx. The hyoid bone is not directly connected to another bone via a bony articulation.
1. The laryngeal cartilages:
The cartilaginous skeleton consists of the thyroid, cricoid and arytenoid cartilages. The midline epiglottic cartilage acts as a dynamic cover for the larynx and as a valve separating it from the oesophagus. Additionally, three paired cartilages not seen routinely on imaging include the corniculate, cuneiform and triticeal cartilages. With advancing age, the cartilages calcify; hence, detection of invasion of tumours becomes easier. Invasion of the thyroid and cricoid cartilages is considered essential for tumour staging purposes. The arytenoid cartilages and the epiglottis (also considered brown or ‘orange’ cartilages) and the corniculate, cuneiform and triticeal cartilages (also called the small cartilages) are not considered for staging purposes.
The thyroid cartilage consists of two laminae separated by the superior thyroid notch anteriorly. Posteriorly, the two laminae form the superior cornu (which are elongated and narrow and provide attachment to the thyrohyoid ligament) as well as the inferior cornu (which are short and thick and articulate with the cricoid cartilage). The thyroid cartilage is an essential component of the skeletal structure of the larynx. It anchors the epiglottis using the false vocal cords and anchors the true vocal cords to the vocal processes of the arytenoid cartilage of the glottis. Variable and asymmetric calcification/ossification of the thyroid cartilage can make radiologic staging difficult and does not indicate tumour invasion.
The cricoid cartilage serves as the only complete ring which stabilizes the larynx in the axial plane to keep the airway open. It consists of a thin anterior arch and a broad posterior arch exhibiting a ‘signet-ring’ appearance. The lower border separates the larynx from the trachea. Articulation with the arytenoid cartilages (cricoarytenoid joints) is an important anatomical landmark for identifying the true vocal cords, and these joints are also commonly involved in rheumatoid arthritis. The cricoid cartilage exhibits the most consistent calcification/ossification amongst all the laryngeal cartilages.
The arytenoid cartilages are paired, pyramidal cartilages that sit atop the posterior cricoid lamina and have three sets of projections, namely the vocal, muscular and superior processes. The vocal processes are the anteriorly directed mucosal projections that pivot on the ring-like cricoid cartilage and are attached to it by the cricoarytenoid muscles. The muscular processes give attachment to the thyroarytenoid muscles (true vocal cords) from which they span across the larynx. The superior processes are an important anatomical landmark as they lie at the level of the false vocal cords.
The corniculate cartilages, called thus because of their horn-like appearance, rest on top of each of the arytenoid cartilages. The cuneiform cartilages lie lateral and superior to the corniculate cartilages. Both the corniculate and cuneiform cartilages lie within the free margins of the aryepiglottic folds. Small cartilaginous nodules (at times bony in nature), the triticeal cartilages, are frequently found in the lateral thyrohyoid ligament. During swallowing, the epiglottis bends down to meet the corniculate cartilages, sealing the airway to prevent food or saliva from entering the airway.
The epiglottis is a leaf-like midline structure that helps to close down the airway during swallowing. It has a suprahyoid free part projecting posterior to the base of tongue and an infrahyoid fixed part also known as the stalk or petiole (Latin: petiolus). The epiglottis is seen best on sagittal imaging. It gives attachment to two important structures, namely the anterior midline median glosso-epiglottic fold and the two lateral pharyngo-epiglottic folds.
2. The laryngeal musculature:
• The anterior group of muscles comprise the thyrohyoid muscles (also known as the strap muscles), and the cricothyroid muscles extending from the inferior thyroid cartilage to the cricoid cartilage.
• The posterior group of muscles comprises the transverse arytenoid muscles and oblique arytenoid muscles (situated superiorly at level of the upper half of the thyroid cartilage) and the posterior and lateral cricoarytenoid muscles situated inferiorly from the midportion of the thyroid cartilage to the cricoid cartilage.
• The central muscles are the thyroarytenoid muscles, which account for the bulk of the true vocal cords and span the glottic compartment’s supero-inferior extent. The medial fibres of the thyroarytenoid muscle are referred to as the vocalis muscle.
• The linea obliqua is a ridge on the postero-lateral aspect of the thyroid cartilage, which gives attachment to the inferior pharyngeal constrictor muscle.
• Functions of the laryngeal muscles:
a. Cricothyroid muscles: rotation of the thyroid cartilage towards the cricoid, lengthening and tensing of the vocal ligaments.
b. Thyroarytenoid and vocalis muscles: shortening and relaxing the vocal ligaments.
c. Posterior cricoarytenoid muscles: abduction of the vocal ligaments.
d. Lateral cricoarytenoid muscles: adduction of the vocal ligaments.
e. Transverse and oblique arytenoid muscles: adduction of the vocal ligaments.
3. The laryngeal membranes:
• Extrinsic membranes which attach components of the larynx to the external structures: thyrohyoid membrane extending between the hyoid bone and thyroid cartilage is pierced by two important structures: the internal branch of the superior laryngeal nerve (branch of the vagus nerve) and the superior laryngeal artery (branch of the external carotid artery). It is vital to contain the exophytic spread of tumours into the neck soft tissues but can also be breached by increasing pressure within a laryngocele.
• Intrinsic membranes which hold the cartilages of the larynx together as a functional unit and act as substantial connective tissue barriers to spread of cancer:
These include:
a. Quadrangular membrane (QM) presents as a curtain of fibrous tissue within the mucosa of the supraglottic larynx extending from the lateral margin of epiglottis/aryepiglottic folds to the arytenoid cartilages/false vocal cords (separating the supraglottic larynx from the hypopharynx). The free superior margin forms the aryepiglottic ligament beneath the aryepiglottic folds, and the free lower margin represents the ventricular/vestibular ligament under the false vocal cords.
b. Conus elasticus (CE) is a fibroelastic membrane extending from the free medial edge of the true vocal cords above to the cricoid cartilage below and is < 1 mm thick. The thickened free superior border forms the vocal ligament (the skeleton of the true vocal cord). The laryngeal ventricle separates the vocal ligament and the ventricular ligament.
4. The laryngeal ligaments:
• The midline hyoepiglottic ligament attaches the epiglottis to the hyoid bone and is covered by a mucosal fold (median glosso-epiglottic fold), which lines the ligament and bifurcates the vallecular region symmetrically. The two lateral pharyngo-epiglottic folds separate the vallecula (oropharynx) from the supraglottic larynx.
• Lateral thyrohyoid ligaments are situated posterolaterally between the hyoid bone and the thyroid cartilage and a midline median thyrohyoid ligament, which is the condensation of the thyrohyoid membrane as it curves around anteriorly.
• The median cricothyroid ligament which represents the anterior midline condensation of the fibres of the cricothyroid muscles, conus elasticus connecting the inferior border of the thyroid cartilage to the cricoid cartilage.
• Cricotracheal ligament.
5. Innervation of the larynx: sensory and motor innervation by the vagus nerve.
• Superior laryngeal nerve: This nerve originates from the inferior ganglion of the vagus nerve. The internal branch pierces the thyrohyoid membrane and provides sensory innervation to the mucosa of the larynx. The external branch does not enter the endolarynx and provides motor innervation to the cricothyroid muscle.
• Recurrent laryngeal nerve: Primarily descends and then ascends in the trachea–oesophageal grooves lying lateral to the cricothyroid joints. On the right side, the recurrent laryngeal nerve loops around the innominate artery, and on the left side, the recurrent laryngeal nerve loops around the aortic arch traversing through the aortopulmonary window.
6. Lymphatic drainage of the larynx and hypopharynx:
The supraglottic larynx develops from the primitive buccopharyngeal anlage (the fourth branchial arch), which is lush with lymphatics. Therefore, a cancer in this region often presents with nodal metastasis. The glottis and subglottis develop from the tracheobronchial buds (glottis from the fifth branchial arch and subglottis from the sixth branchial arch), which have sparse lymphatics and hence have lesser propensity towards nodal metastasis.
Nodal drainage stations
• Supraglottis: Generally, drains in a cephalad direction with the preepiglottic space containing abundant lymphatic tissue. Primary drainage (first station) is to the intralaryngeal nodes and subsequently (in the decreasing order of occurrence) to Level II, III, IB and retropharyngeal group. Lymphatic drainage is to the bilateral stations in epiglottic cancers.
• Glottis: Level IV/VI, Delphian node (anterior to the cricothyroid membrane) and parathyroid region nodes
• Subglottis: pre- and paratracheal, superior mediastinal nodes
• Pyriform sinuses: Level II, III, IV nodal stations.
• Posterior hypopharyngeal wall: Level III, IV, VI nodal stations and retropharyngeal nodes
• Postcricoid region: Level III, IV, VI nodal stations
Similar size criteria for different levels, node morphology and extracapsular spread; carotid encasement needs to be documented as in other head neck cancers. There is a higher incidence of nodal metastasis with associated extralaryngeal spread and cartilage invasion.
1. Supraglottis: is the largest compartment of the larynx and extends from the lateral pharyngo-epiglottic folds above to the inferior margin of the laryngeal ventricle below.
Structures to be identified in this compartment include the following:
• Epiglottis:
• Hyoepiglottic ligament: Visualized as the midline median glosso-epiglottic fold.
• Preepiglottic space (PES): C-shaped fat-containing structure, critical as small infiltrative cancers, can lie undetected until they grow to a significant size.
• Para-glottic space (PGS): Linear fat-containing structures seen as inferior continuation of the preepiglottic space. Both PES and PGS play an important role in staging and disease prognosis
• Aryepiglottic folds (AE folds): Fat-containing structures projecting from the lateral margins of the epiglottis above to the tips of the arytenoid cartilages below. They separate the supraglottic larynx from the hypopharynx as they form the superolateral borders of the supraglottis and the anteromedial margin of the pyriform sinuses (part of the hypopharynx). The AE folds are one of the two ‘shared walls’ between the larynx and hypopharynx. Tumours arising from these structures are called marginal tumours based on the vector of spread. An anteromedial vector of spread results in a supraglottic laryngeal mass, whereas a posterolateral spread results in a hypopharyngeal mass.
• False vocal cords (FVCs): Inferiorly, the aryepiglottic folds turn upwards on themselves, forming the false vocal cords which represent the mucosal surface of the supraglottic laryngeal airway. The level of the FVC can be definitively ascertained by identifying the hypodense/hyperintense (on CT/T1W MR sequence) fat as these structures are inferior continuation of the fatty AE folds and by identifying the superior processes of the arytenoid cartilages. The free margin of the FVC is the ventricular ligament.
• Vestibule: It is the airway of the supraglottic larynx.
• Quadrangular membrane (QM): As it represents a continuous sheet of fibrous tissue within the mucosa of the supraglottic larynx, it is generally not visualized by any imaging technique.
• Ventricle: It is the small horizontally oriented air space between the FVC and the true vocal cords and forms the inferior border of the supraglottis.
2. Glottis: is the smallest section of the larynx extending from the inferior border of the laryngeal ventricle to the inferior margin of the true vocal cords with a maximum craniocaudal extent of approximately 10 mms.
Structures to be identified in this compartment include:
• True vocal cords (TVCs): Comprising the thyroarytenoid muscle and its medial fibres (vocalis muscle). The free margin of the vocalis muscle is the vocal ligament over which is the mucosal lining. Reinke space is a potential space between the vocal ligament and the overlying mucosal lining. It is a potential space of the superficial lamina propria of the vocal cord that contains a loose fibrous matrix and has sparse lymphatics.
• Anterior commissure (AC) and posterior commissure (PC): The AC is the anterior midline meeting point of the true vocal cords and can be adequately visualized only during quiet respiration. The PC is the mucosa overlying the portion of the cricoid cartilage between the arytenoid cartilages. The thickness of the soft tissue in the region of both AC and PC should not be more than 1 mms on CT/MRI images obtained in quiet respiration.
• Broyles ligament (tendon of the anterior commissure): Connects the true vocal cords to the thyroid cartilage. It penetrates the thyroid cartilage and carries blood vessels and lymphatics within its fibrous tissue. In this way, the Broyles ligament serves as a route to the extralaryngeal spread of the cancer. This is further aided by the fact that the central area of the thyroid cartilage is devoid of perichondrium. The laryngeal ventricle also opens into this space.
3. Subglottis: An overlooked, but very important subsite extending from the undersurface of the true vocal cords above till the undersurface of the cricoid cartilage below where the laryngeal airway assumes an oval to round shape.
Structures to be identified in this compartment include:
• Mucosal lining closely related to the underlying perichondrium without any intervening soft tissue thickening.
• The cricothyroid joints. The trachea–oesophageal grooves lie posteromedial to these structures and act as markers for the course of the recurrent laryngeal nerves.
• Conus elasticus (CE) forms the lateral border of the subglottic region and is generally not visualized by any imaging technique.
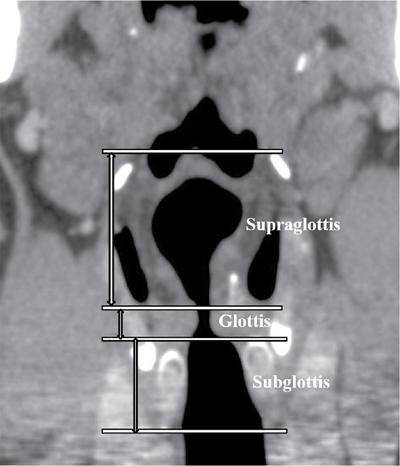
Fig. 3.11.7Coronal CT image depicting the subsites of the larynx.
1. The pyriform sinuses: are symmetric pouches hanging behind the larynx. The anteromedial margins of the pyriform sinuses are the posterolateral walls of the supraglottic aryepiglottic (AE) folds. The inferior tip of the pyriform sinus, or pyriform apex, lies at the level of the true vocal cords (TVCs).
2. The posterior hypopharyngeal wall (PHW) is the inferior continuation of the posterior oropharyngeal wall, extending from the level of the hyoid bone above to the inferior cricoid cartilage margin below.
3. Postcricoid region (PCR) is the anterior wall of the lowermost portion of the hypopharynx, extends from the level of the cricoarytenoid joint to the cricopharyngeus muscle/lower border of the cricoid cartilage and comprises the mucosa covering the posterior surface of the cricoid cartilage. It is the interface between the hypopharynx and the larynx anteriorly and cervical oesophagus inferiorly and one of the most challenging sites to delineate on CT or MRI. The PCR is the second of the two ‘shared walls’ between the larynx and hypopharynx, but is considered as a hypopharyngeal site.
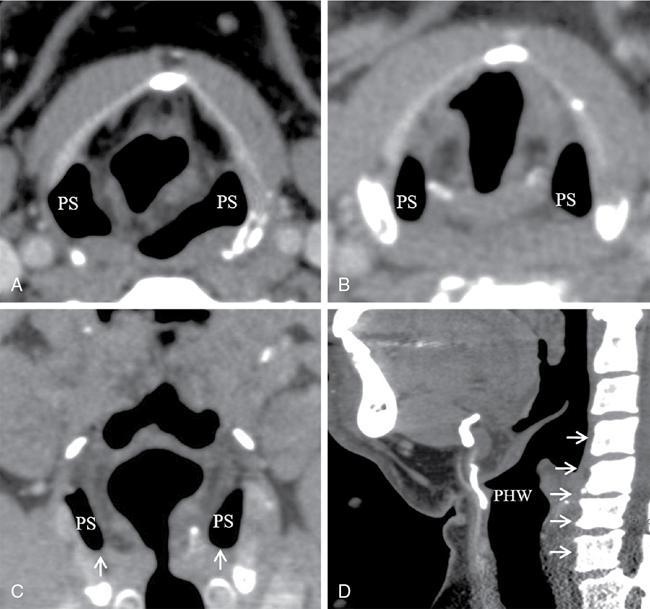
Fig. 3.11.8Axial (A,B), coronal (C) and sagittal (D) CT images depicting the subsites of the hypopharynx. PHW, posterior hypopharyngeal wall ( horizontal arrows); PS, piriform sinus. Note that the apex of the piriform sinuses lies at the level of the true vocal cords ( vertical arrows). The posterior hypopharyngeal wall is the continuation of the posterior oropharyngeal wall from above ( arrows) and extends inferiorly till junction of the posterior hypopharynx and cervical oesophagus (inferior margin of the cricoid cartilage).
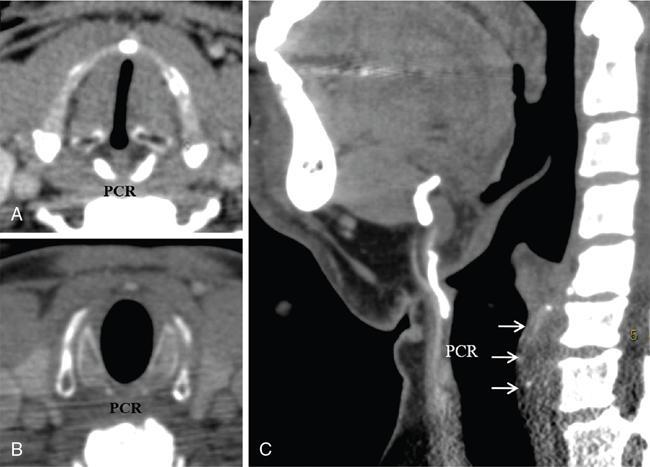
Fig. 3.11.9Axial (A,B) and sagittal (C) CT images depicting the subsites of the hypopharynx. PCR, postcricoid region ( arrows).
Reading a larynx/hypopharynx imaging study (CT/MRI):
Multiplanar imaging: Correlation of normal and pathological structures in axial, coronal and sagittal planes help in understanding the anatomy and interpretation of abnormal findings.
Angulated axial images must be reconstructed along the ‘laryngeal plane’, i.e., the plane that corresponds most to the plane of the laryngeal ventricle (Fig. 3.11.10). True axial sections may cause spatial distortion and lead to interpretive errors.
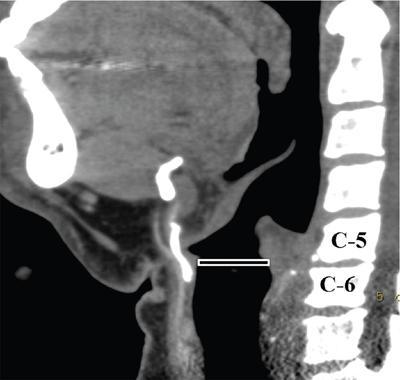
Fig. 3.11.10Sagittal CT image depicting the ‘laryngeal plane’ ( line), a plane that most closely approximates the plane of the laryngeal ventricle and is, in most cases, parallel to the plane of the C5–C6 intervertebral disc space and must be oriented perpendicular to the plane of the airway.
As far as possible, an axial section that passes through the C5–C6 disc space and is perpendicular to the airway meets the requirements. The coronal reconstructions can be obtained perpendicular to the axial images together with true sagittal reconstructions of the airway and surrounding soft tissues.
Imaging issues in the larynx and hypopharynx:
a. Assessment of the full extent of a mucosal lesion is not possible.
b. Anatomical appearances of structures of the airway change in different phases of respiration
c. Variability in cartilage ossification and calcification
d. Asymmetric appearance of aryepiglottic folds and pyriform sinuses can be a normal finding, and symmetric involvement of the epiglottis by pathology can be neglected and overlooked.
e. Imaging cannot definitively comment on cord mobility.
Standardized levels of reading an axial larynx/hypopharynx imaging study (CT/MRI):
It is essential to be well acquainted with the standard levels of reading an axial imaging study and identify all structures in that specific region (Figs 3.11.11–3.11.15). The relative location and extent of the intrinsic laryngeal membranes, i.e., the quadrangular membrane and the conus elasticus not visualized on imaging, have been depicted in Fig. 3.11.16.
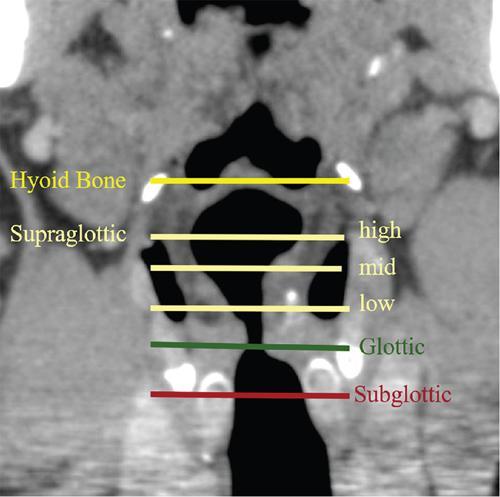
Fig. 3.11.11Coronal CT image showing the six standardized levels ( lines) of reading and identifying normal anatomical structures on sequential axial CT images.
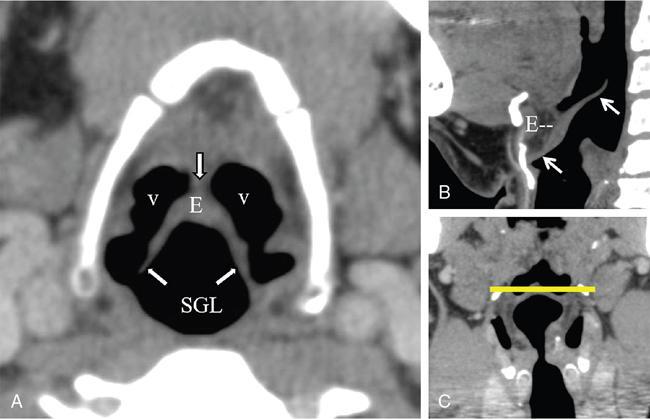
Fig. 3.11.12Hyoid bone level. Axial (A), sagittal (B) and coronal reference (C) CT images. The epiglottis (E) which has a suprahyoid free margin and an infrahyoid fixed part ( upper and lower arrows in B). Midline hyoepiglottic ligament represented by the median glossoepiglottic fold ( vertical arrow) which attaches the epiglottis to the hyoid bone bisects the vallecular region (v). The two lateral pharyngo-epiglottic folds ( oblique arrows) separate the valleculae from the supraglottic larynx (SGL).
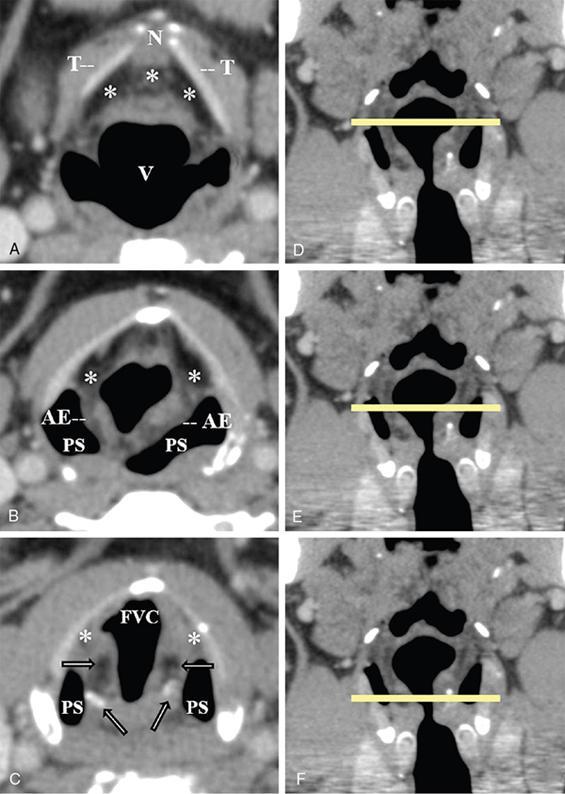
Fig. 3.11.13Supraglottic level (high, mid and low). Axial CT images at preepiglottic space level (A), aryepiglottic fold level (B) and false vocal cord level (C) with corresponding coronal CT reference images (D–F). Preepiglottic fat is a C-shaped fat containing structure ( asterisks in A) continuous inferiorly with the paraglottic fat ( asterisks in B,C). The two laminae of the thyroid cartilage (T) fuse in the midline anteriorly and form the superior thyroid notch (N). Airway of the SGL is represented by the vestibule (V). The aryepiglottic folds (AE) and piriform sinuses (PS) are well seen. AE folds separate the SGL from the hypopharynx (B). The false vocal cord (FVC) level (C) is identified by the presence of fat ( horizontal arrows) and the superior processes of the arytenoid cartilage ( oblique arrows).
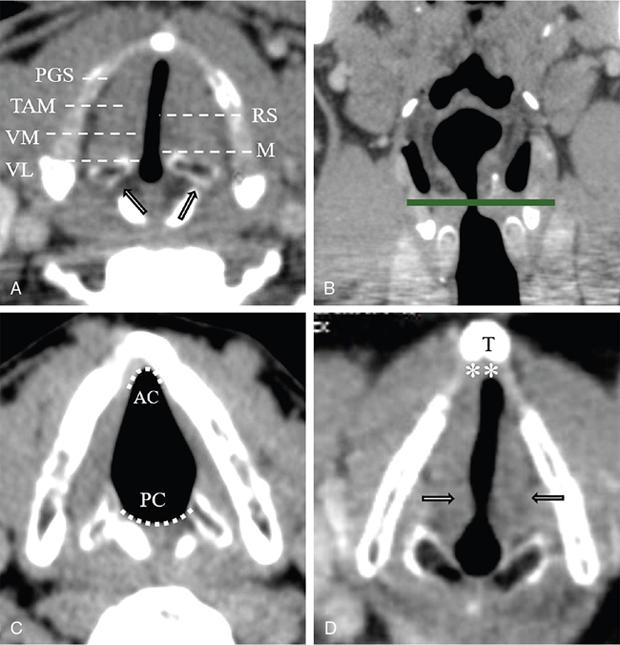
Fig. 3.11.14Glottic level. Axial CT images at glottic level (A,C,D) with corresponding coronal CT reference image (B). The true vocal cord (TVC) level (A) is identified by the presence of thyroarytenoid muscle (TAM) and the crico-arytenoid joints ( oblique arrows). The structures that can be identified from lateral to medial on axial images at this level include PGS, para-glottic space; RS, Reinke space; M, the mucosal lining; TAM, thyroarytenoid muscle; VL, vocal ligament; VM, vocalis muscle. Curved dotted lines (C) represent the anterior commissure (AC) and the posterior commissure (PC). Asterisks (D) represent the site of attachment of the Broyle ligament connecting the true vocal cords ( arrows) to the thyroid cartilage (T).
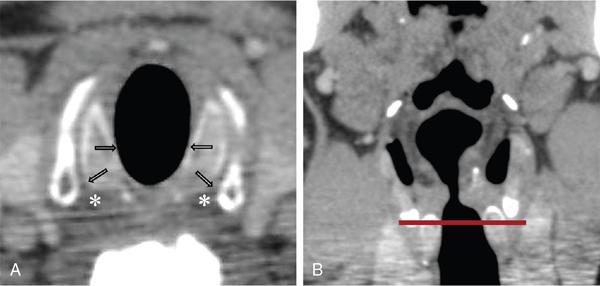
Fig. 3.11.15Subglottic level. Axial CT image at the subglottic level (A) with corresponding coronal CT reference image (B) shows the oval shape of the laryngeal airway till the undersurface of the cricoid cartilage with the mucosa remaining closely attached to the underlying perichondrium ( horizontal arrows). The trachea-oesophageal grooves ( asterisks) are situated postero-medial to the crico-thyroid joints ( oblique arrows) and are important anatomical landmarks to identify course of the recurrent laryngeal nerves.
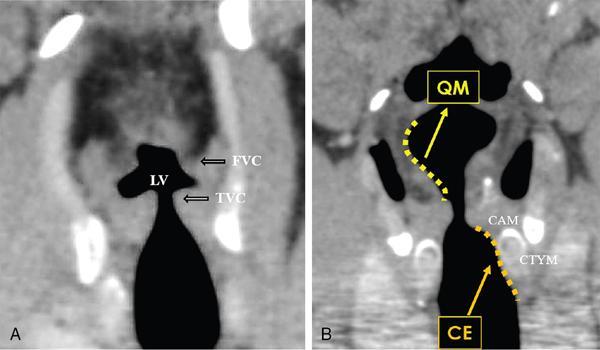
Fig. 3.11.16Coronal CT image (A) depicting the laryngeal ventricle (LV) between the false vocal cord (FVC) above and the true vocal cord (TVC) below. Coronal CT image (B) depicts in free-form dotted curved lines the projected positions of the quadrangular membrane (QM) and the conus elasticus (CE). These structures are not visualized on imaging. The crico-arytenoid muscle (CAM) and the crico-thyroid muscle (CTYM) are identified superiorly and inferiorly, respectively.
These standardized levels are as follows:
• At the level of the hyoid bone.
• Supraglottic level: This is the largest compartment and is evaluated at three levels: high, mid and low.
• Glottic level: Structures comprising the true vocal cord from lateral to medial (periphery to centre) are PGS, thyroarytenoid muscle, vocalis muscle, vocal ligament, Reinke space and mucosal lining.
• Subglottic level.
Only gold members can continue reading. Log In or Register to continue