Childhood primary tumors of the liver are rare. Of these, about two thirds are benign and one third malignant (1). The incidence varies from geographic region to region. According to the Surveillance, Epidemiology and End Results (SEER) data, between 1973 and 1977 and 1993 and 1997, hepatoblastoma rates increased (from 0.6 to 1.2/1,000,000), while hepatocellular carcinoma rates decreased (from 0.45 to 0.29/1,000,000) (2). The most common tumors according to histopathology are hepatoblastoma (HBL), hepatocellular carcinoma (HCC), benign vascular tumor, mesenchymal hamartoma, and sarcoma (Table 14.1) (1). Benign tumors are usually found incidentally as an asymptomatic abdominal mass. Malignant tumors usually present with abdominal distension with or without a palpable abdominal mass. Children with both HBL and HCC may also present with weight loss, fever, and anorexia. Anemia, thrombocytopenia, and leukocytosis are sometimes associated findings.
Complete surgical resection is the standard curative treatment for malignant tumors. Chemotherapy, radiotherapy, and local ablation treatment are adjunctive to surgery or palliative for incurable patients.
Computed tomography (CT) and magnetic resonance imaging (MRI) are the most definitive diagnostic tests and can often help to differentiate benign from malignant tumors preoperatively.
Table 14.1 Incidence of Primary Hepatic Tumors in Childhood
Tumor
Number of Patients
Percentage
Hepatoblastoma
532
43
Hepatocellular carcinoma
284
23
Benign vascular tumor
166
13
Mesenchymal hamartoma
75
6
Sarcoma
79
6
Adenoma
22
2
Focal nodular hyperplasia
22
2
Miscellaneous
57
5
Adapted from Weinberg AG, Finegold MJ. Primary hepatic tumors of childhood. Hum Pathol. 1983;14(6):512-537.
BENIGN TUMORS
Vascular Tumors
The most common benign lesions in children are hemangiomas and hemangioendotheliomas. Hemangiomas are the most common benign liver tumors and usually occur within the first 6 months of life (3). Most hemangiomas are incidentally discovered on imaging studies. Infantile hemangioendothelioma is a subtype of hemangioma that is typically found in infants. A female predilection is noted, with a female-to-male ratio of 4.3:1 to 2:1. Afflicted infants generally present with abdominal distension and cutaneous hemangiomas (10% of cases) that suggest the diagnosis. More than 50% of these infants have high-output cardiac failure at initial presentation (3). Classical triad of hepatomegaly, anemia, and congestive heart failure leads to the suspicion of infantile hemangioendothelioma. Kasabach-Merrit syndrome with consumptive coagulopathy, thrombocytopenia, and hemorrhage is the leading cause of morbidity and mortality seen in infantile hemangioendothelioma (4).
The natural history for hemangiomas is spontaneous regression in the first 2 years of life; however, treatment is required if cardiac failure or platelet consumption occurs. Several treatment options are available, including high-dose corticosteroids (3-5 mg/kg/day), interferon-alfa (3 million U/m2/kg/day SC), aminocaproic acid, vincristine, and cyclophosphamide, all are associated with potential severe side effects and poor outcome (5). Focal lesions can be treated with complete surgical excision. Selective hepatic artery embolization may not be as successful for multifocal as it is for focal lesions. Operative ligation of the hepatic artery can also be used to decrease shunting through the lesion, with subsequent improvement in cardiac output (6). Radiation therapy is usually avoided because angiosarcomatous degeneration may follow radiation. Rarely, liver transplantation may be indicated for diffuse disease that is unresponsive to steroid and interferon therapy.
Mesenchymal Hamartoma
Infantile mesenchymal hamartomas are rare benign tumors, comprising 6% of liver tumors in children (Table 14.1), and can be considered more of a malformation than true tumors. They tend to be diagnosed before the age of 2 years, more common in the right lobe of the liver. They usually present as an asymptomatic abdominal mass after a period of rapid growth during the first few months of life and cause compression of adjacent tissue but are curable by resection (7). Alpha-fetoprotein (AFP) levels may be variably elevated. CT scan reveals a well-circumscribed, multilocular, heterogeneous, cystic mass with solid septa and stroma. Biopsy is recommended if cysts are small or appear more solid rather than septated. Complete surgical excision, with a rim of normal tissue (if possible), is the treatment of choice (8).
Focal Nodular Hyperplasia and Hepatic Adenomas
Focal nodular hyperplasia (FNH) and hepatic adenomas are rarely seen in children. Both of these benign lesions have an association with a high-estrogen environment and frequently occur in adolescent girls. Hepatic adenomas are associated with oral contraceptive use. Signs and symptoms may be absent or are nonspecific and include abdominal pain and mass symptoms. A characteristic central stellate scar on CT scan is pathognomonic for FNH. A triphasic helical CT scan is the optimal study to make the diagnosis of FNH. Differentiating FNH from adenomas may require a technetium sulfur colloid scan, which reveals uniform uptake by FNH lesions. Patient suspected of FNH should be managed conservatively. If a diagnosis remains unclear, a liver biopsy may be helpful. If the lesion becomes symptomatic or rapidly enlarging, complete surgical resection may be necessary to differentiate FNH from malignant tumors (8,9).
PRIMARY MALIGNANT LIVER TUMOR
Children with primary malignant liver tumors (PMLTs) often present with an abdominal mass or generalized abdominal enlargement. The child may have pain localized to the right upper quadrant, fever, anorexia, weight loss, jaundice, or vomiting. The first presentation may, on occasion, be an acute abdominal crisis caused by tumor rupture and hemoperitoneum. Paraneoplastic syndrome, such as precocious sexual development, has been associated with PMLTs (10). Anemia and thrombocytosis often occur. This is probably related to the ability of HBL cells to secrete gonadotropin, interleukin-1B, which induces IL-6 production in fibroblasts of endothelial cells (11,12).
Hepatoblastoma
HBL is the most common PMLT occurring in the first 20 years of life and accounts for 1% of all pediatric malignancies and about 60% of PMLTs in the pediatric age group (10,13,14). Median age at diagnosis is 16-19 months. Only 5% of the cases occur in children older than 4 years. As with all PMLTs, there is a male predominance (1,15). HBL has been reported to be associated with a host of conditions, including Beckwith-Wiedemann syndrome, Wilms tumor, adrenal cortical tumors, fetal alcohol syndrome, familial adenomatous polyposis (FAP), prematurity, low birth weight, precocious puberty in boys caused by human chorionic gonadotropin secretion, and thrombocytosis (11,14, 15, 16, 17, 18). The cell of origin is thought to be a pluripotent hepatic stem cell (19).
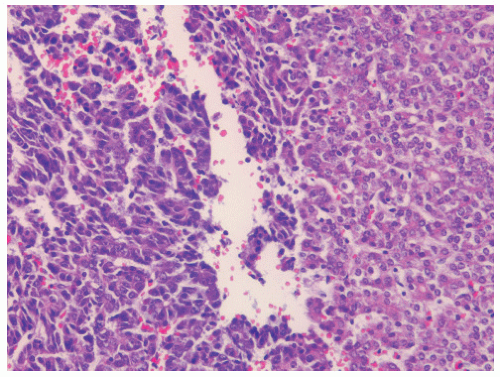
HBL may be histologically classified into six patterns (Table 14.2). Conventional HBLs contain fetal hepatoblasts, embryonal hepatoblasts, or a mixture of the two cell types (Figs. 14.1 and 14.2). Fetal-type hepatoblasts recapitulate the cytoarchitecture of the normal human fetal liver. Cells of the early fetal liver and the cells of fetal HBL are of similar size and configuration. Both proliferate as cuboidal cells with trabeculae one- to two-cell thick. Both display strong positivity for AFP. Both tissues also display sinusoidal hematopoiesis and a lack of intrahepatic bile ducts (20). Fetal cells are slightly smaller than normal hepatocytes and have a low nucleocytoplasmic ratio. In contrast, embryonal hepatoblasts have a higher nucleocytoplasm ratio than do fetal cells, and they also have a compact basophilic cytoplasm (Fig. 14.3). This gives a light-microscopic impression of a higher cell density (1,21, 22, 23). Small-cell undifferentiated or anaplastic HBL contains sheets and nests of medium-sized cells, with little or no evidence of hepatoblastic differentiation. There is scant cytoplasm and a high mitotic index. Mixed epithelial and mesenchymal HBL is composed of typical areas of fetal epithelial and embryonal type cells mixed with primitive mesenchyme and various mesenchymally derived tissues (24).
Table 14.2 Histologic Classification of Hepatoblastoma
Conventional epithelial type (56%)
Mixed epithelial and mesenchymal type (44%)
Fetal pattern (31%)
Without teratoid features (34%)
Embryonal and fetal pattern (19%)
With teratoid features (10%)
Macrotrabecular pattern (3%)
Small-cell undifferentiated pattern (3%)
Modified from Jon M. Rowland. Hepatoblastoma: Assessment of criteria for histologic classification. Med Pediatr Oncol. 2002; 39(5):478-483.
Figure 14.1 Hepatoblastoma, ×20 magnification. (Courtesy Dr John Buchino.)
Figure 14.2 Hepatoblastoma, ×40 magnification. (Courtesy Dr John Buchino.)
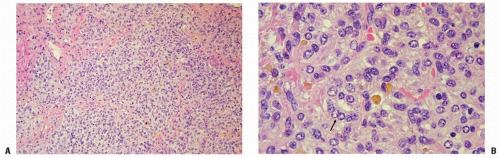
Figure 14.3 Hepatoblastoma. A: Fairly well-defined tumor cells arranged in a trabecular pattern and composed predominantly of cells with fetal hepatocyte differentiation pattern. There are trabeculae of cuboidal cells that contain small round nucleus with fine nuclear chromatin and an indistinct nucleolus. The cytoplasm varies from eosinophilic to clear and contains many pigment deposits (hematoxylin and eosin ×100). B: A second population of small ovoid cells is arranged in clusters. These cells are of embryonal origin (arrow) (hematoxylin and eosin ×400).
It is unclear whether the recognized histologic subtypes are related to prognosis. The subtypes can occur together within the same tumor in varying composition (25). Some investigators report that in long-term survivors of HBL, the most common histology is the conventional type, with a predominantly fetal cell pattern (31). However, there is no uniformly accepted definition of “predominantly” or “pure” fetal histology (26). Although conventional epithelial tumors constitute 60% of all HBLs, they represent 85% of HBLs in children who have undergone complete tumor resection and are long-term survivors (1,22). Almost no children with anaplastic HBL survive the disease. A Pediatric Oncology Group (POG)-Children’s Cancer Study Group (CCSG) trial showed the distinction between fetal HBL and other histologic subtypes to be of prognostic importance in stage I disease (3-year progression-free survival of 79% vs. 56%, p = 0.11) (27). However, not all investigators have confirmed the prognostic importance of histologic subtypes in all stages (21). For example, a large analysis the Japanese Study Group for Pediatric Liver Tumor (JPLT) found no significant influence of HBL histologic classification on outcome (28).
Hepatocellular Carcinoma
HCC, the second most common PMLT in children, accounts for about one fourth to one third of pediatric hepatic malignancies (10). HCC is unusual in children younger than 5 years. The median age of presentation for pediatric HCC is 10-12 years (10,29, 30, 31). Approximately 25% of cases in children are associated with cirrhosis (31). Causes that lead to cirrhosis include biliary atresia, Fanconi anemia, glucose-6-phosphatase deficiency, and hereditary tyrosinemia. HCC has also been reported in association with hemihypertrophy, anomalies of the abdominal venous drainage system, and the use of oral contraceptives. HCC occurs in areas with a high prevalence of hepatitis B viral infection (32). The association of maternal HBsAg seropositivity in children with HCC may be up to 94% in endemic area (32), though the hepatitis B carrier status varies by geographic area. Molecular hybridization studies have shown that viral DNA is integrated into the DNA of cellular lines derived from human HCC and also into morphologically nonmalignant adjacent liver cells (10). Implementation of universal hepatitis B vaccination program starting in 1984 in Taiwan has lead to a remarkable decreasing incidence of childhood HCC from 4.5 per 100,000 in 1981-1984 to 1.9 per 100,000 in 1990-1996, indicating the value of hepatitis B immunization as an effective means of controlling HCC (33).
There is a fibrolamellar (FL) histologic variant of HCC, which occurs in the noncirrhotic livers of older children. This variant is characterized by large polygonal neoplastic hepatocytes and lamellar bundles of collagen. Although patient numbers are small, some think that this tumor is associated with a higher frequency of resectability and a good probability of cure. However, others have failed to demonstrate a favorable outcome of the FL variant in children (8,10,16,21,34).
Undifferentiated Embryonal Sarcoma of the Liver
Undifferentiated embryonal sarcoma of the liver is the third most common liver malignancy in children and adolescents, comprising 9-13% of liver tumors. Most are diagnosed at the age of 5-10 years. It may be solid or cystic on imaging, frequently with central necrosis. Distinctive features are characteristic intracellular hyaline globules and marked anaplasia in a mesenchymal background (20).
Embryonal rhabdomyosarcoma arises from bile ducts and usually occurs in children younger than 5 years. It may share some common clinical and pathologic features with undifferentiated embryonal sarcoma of the liver. Clinically, undifferentiated embryonal sarcoma of the liver tends to occur in older children, often arises in the right lobe of the liver, and does not present with jaundice or biliary obstruction, while bile duct rhabdomyosarcoma occurs more frequently in younger age (median 3.4 years), arises in hilar area, and presents with more jaundice than the former. Surgery alone may achieve local control for undifferentiated embryonal sarcoma of the liver, while surgery and radiotherapy are required for bile duct rhabdomyosarcoma. Chemotherapy regimens used to treat the former differ from those used to treat bile duct rhabdomyosarcoma (35).
DIAGNOSIS
If a hepatic or biliary tumor produces biliary obstruction, there may be elevations of serum hepatic enzymes or bilirubin (36,37). An abdominal ultrasound examination helps to establish the presence of a hepatic mass and differentiates cystic from solid lesions. Ultrasound permits evaluation of the adrenals and the kidneys, helps to exclude these organs as possible primary sites of tumor metastatic to the liver, and allows evaluation of the inferior vena cava for tumor thrombus. Color Doppler ultrasound may be performed to demonstrate the relationship of the tumor to hepatic vessels (38). The technetium-90m sulfur colloid scan is of some value in localizing the tumor to the liver and defining its boundaries. It is a sensitive test, but not specific. CT and MRI provide superior delineation of the mass and show evidence of multifocality (39). On nonenhanced CT, epithelial HBL is a homogeneous low-attenuation mass. The mixed type is inhomogeneous. Calcifications can be present. Contrast enhancement of the periphery or septa may be seen. On MRI, the epithelial type is homogeneous and hypointense on T1 and hyperintense on T2. The mixed type may be more inhomogeneous and hypointense on T1 and T2, and hemorrhage will show high signal intensity on T1 and T2 (Fig. 14.4). On CT, HCC will show solitary or multiple masses. Calcification can occur. The tumor rim may show enhancement with contrast. On MRI, the T1 images may be isointense or hyperintense. On T2 images, a mosaic pattern (caused by necrosis, hemorrhage, septa, and fatty metaplasia) is common (29). The operating surgeon may request an angiogram to obtain information about the origin and distribution of the right and left hepatic arteries to provide additional information on the vascular supply of the tumor (10). Routine chest radiographs and thoracic CT scans are necessary because 10-20% of patients with HBL and 30% of patients with HCC have lung metastasis at the time of diagnosis (12,18,40,41). Positron emission tomography CT holds promise for better surgical outcomes and greater sensitivity for residual or relapsed disease (42).
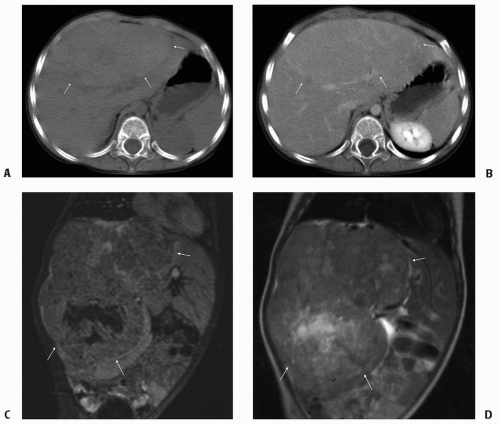
Figure 14.4 A-D: Hepatoblastoma is best visualized on cross-sectional imaging. It is homogeneous and hypointense on T1 and hyperintense on T2 on magnetic resonance images.
A valuable test in evaluating PMLT is the serum AFP. The clinician should note that AFP, synthesized by the fetal liver, may be elevated in pregnant women. AFP levels are high in the normal newborn infant but drop rapidly by the age of 1 month. AFP should be barely detectable by the age of 2 years (18). Approximately two thirds of children with HBL and HCC have an elevated AFP (37). However, the clinician should be cautioned that AFP is not always elevated in HBL or HCC and that this protein may be slightly elevated in benign hamartomas. Absence of AFP elevation may be a poor prognostic sign in HBL; it is associated with the small-cell (anaplastic) histologic type and responds poorly to therapy. For patients with elevated AFP, it may be of value in monitoring the course of therapy (38). Complete resection of HBL or HCC should result in a normal AFP by 2 months postoperatively (17). No change in an elevated AFP after surgery indicates either residual tumor or regenerating normal liver. The diagnosis of growing tumor depends on confirmatory imaging studies. An elevation in the AFP during the follow-up period generally heralds a local tumor recurrence or distant metastasis (37).
Genetic abnormalities are found in HBL. Trisomies 2, 8, and 20 have been reported in tumor samples as well as t (1;4) (q12;34) translocation. The loss of heterozygosity of 11p15 is seen in about one third of cases (12). There is a clear association between HBL and familial adenomatous polyposis (FAP). Germline mutations in APC tumor suppressor gene occur in patients with FAP. One study estimated that 1 in 20 HBLs is probably associated with FAP (43). Increasing data support a role for aberrant transduction of the Wnt/beta-catenin signaling pathway and its molecular targets in HBL tumorigenesis (25,44,45). A study in a mouse model of HBLs induced by toxin exposure detected mutations of the beta-catenin protooncogene in 100% of the tumors analyzed (46). Increasing evidence suggests that HBL is derived from a pluripotent stem cell (19). This supports the hypothesis that such tumor may arise from a developmental error during hepatogenesis. Research particularly focused on these developmental processes governing liver maturation and growth may ultimately lead to more effective targeted therapy for this disease.
There are two major staging systems for PMLT, one is from CCSG and POG (Table 14.3), and the other is from 2002 The American Joint Committee on Cancer (AJCC) TNM staging system (Table 14.4) (48). All are based on resectability and, to a lesser extent, microscopic residual tumor (12,49). Figure 14.5 shows that the International Society of Pediatric Oncology Liver Tumor Study Group (SIOPEL) Pretreatment Extent of Disease (PRETEXT) grouping system divides the liver into four parts (40). The clinician must be wary of the pitfalls in the existing staging systems. There are at least two important drawbacks of some of the systems shown. First, the systems are applied at initial diagnosis. If upfront chemotherapy is given and if it produces a substantive tumor response before surgery, then the initial stage may no longer be pertinent. Second, a surgeon’s determination of resectability is somewhat subjective and varies among practitioners (50).
Table 14.3 Children’s Cancer Study Group and Pediatric Oncology Group Staging System for Primary Malignant Liver Tumors (10,12,38,47)
Stage
Description
I
Complete resection of the tumor
II
Microscopic residual disease
III
Macroscopic residual tumor
IV
Distant metastatic tumor
Only gold members can continue reading. Log In or Register to continue