Chapter 11 Lumbar Transforaminal Epidural Steroid Injection, Infraneural Approach
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
Several approaches can be used for a transforaminal injection. The more traditional subpedicular or supraneural injection is described in Chapter 10. In this chapter, we will describe the infraneural technique, which has also been called the retrodiscal or preganglionic approach.1–3 With this technique, the needle will stay “low in the hole” or in the lower third of the foramen.
This approach can be used in place of the traditional subpedicular, retroneural, or supraneural approach or when anatomic or surgical changes compromise a safe and direct supraneural approach, making it more challenging. In addition, recent literature has questioned the concept of the “safe triangle,” which may suggest that this alternate approach could provide a safer injection, since it may be a less vacular location.1,4,5
This technique is also called the retrodiscal approach because the needle placement is placed just posterior to the disc’s posterior anulus. Inadvertant disc injection may occur due to this close disc proximity. Some authors describe it as the preganglionic approach because the needle tip lies along the transiting nerve root proximal to the DRG.1–35 Because of the more inferior needle tip placement, the injectate tends to flow along the nerve root as it transits inferiorly past a centrally herniated disc. Thus the targeted nerve level for this procedure may be different than for the supraneural technique. Therefore, the infraneural approach may be beneficial for injecting the nerve at the same disc level as a central herniation instead of injecting below as in the supraneural technique.
Of note is that the initial trajectory is quite similar to that used for lumbar discography.
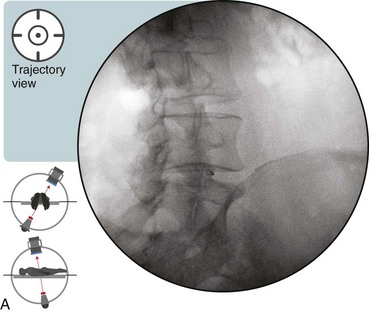
 Trajectory View
Trajectory View
Confirm the level (with the use of the anteroposterior view) before obtaining the trajectory view.
Tilt the fluoroscope to optimize endplate visualization.
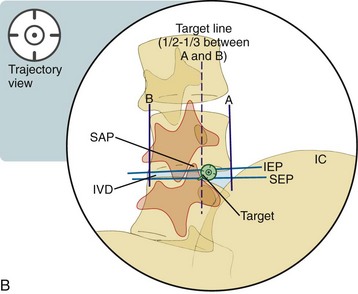
 A caudad or cephalad tilt is used to line up both the superior endplate (SEP) and the inferior endplate (IEP) of the adjacent lumbar vertebrae. (Preferentially line up the SEP interior to the target.)
A caudad or cephalad tilt is used to line up both the superior endplate (SEP) and the inferior endplate (IEP) of the adjacent lumbar vertebrae. (Preferentially line up the SEP interior to the target.)
Oblique the fluoroscope ipsilaterally (Figures 11-1 and 11-2):
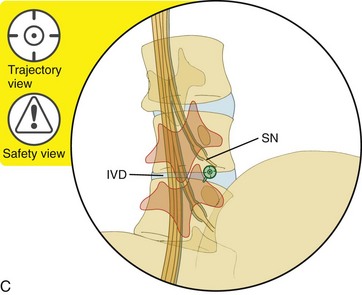
 Trajectory View Safety Considerations
Trajectory View Safety Considerations
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


