Lung carcinoma is the most common fatal malignancy in both men and women. In the United States, it accounts for 14% to 15% of all new cancers and 26% to 30% of all cancer deaths. Lung cancer is more common in men than women, but at present its incidence is decreasing in men and increasing in women.
RISK FACTORS FOR LUNG CANCER
Tobacco smoking accounts for 80% to 90% of lung cancers. In smokers, the risk of lung cancer correlates with younger age at the onset of smoking, the duration and cumulative amount of exposure, and the depth of inhalation. Heavy smoking is associated with a 20- to 30-fold increase in lung cancer risk compared to nonsmokers. A decrease in risk following smoking cessation has been demonstrated. Well-differentiated squamous cell carcinoma, small cell carcinoma, large cell carcinoma, and to a lesser extent adenocarcinoma all demonstrate an increased incidence with increasing cigarette consumption. About 25% of lung cancers in nonsmokers have been attributed to second-hand smoke.
Increasing age is associated with an increased risk of lung cancer. Lung cancers are rare in patients under age 30.
Occupational exposures to various substances have been linked to lung cancer; as many as 10% of lung cancer cases may be due to occupational exposure. Agents associated with occupational lung cancer include arsenic, nickel, chromium, asbestos, beryllium, cadmium, chromium, mustard gas, pesticides, and radon or uranium.
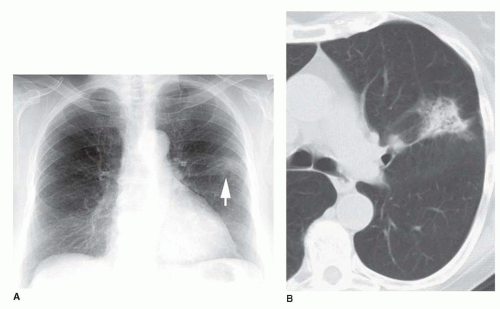
Asbestos exposure is the best-recognized occupational risk for lung cancer and is the most frequent exposure in the general population (Fig. 3-1). A dose-response relationship between the severity and duration of asbestos exposure and the likelihood of developing lung cancer is well established, although the risk of exposure depends not only on the amount of asbestos to which one is exposed but also the fiber type (increased risk with amphibole fibers), the industrial use of asbestos, the conditions of exposure, and the presence of asbestosis. The risk of lung cancer in a heavily exposed asbestos worker is about five times that of a nonexposed subject. Also, smoking is a synergistic risk in asbestos-exposed subjects: the risk of lung cancer in an asbestos worker who is a heavy smoker is about 20 times that of a nonsmoking asbestos worker and 100 times that of a nonexposed nonsmoker (Table 3-1).
Diffuse pulmonary fibrosis has been associated with a 10-fold increase in the risk of lung cancer. In addition, patients with focal lung scarring, particularly as a result of tuberculosis, can develop a carcinoma in association with areas of fibrosis or scarring. Although this is infrequent, cases of carcinoma arising in areas of focal scarring, so-called scar carcinoma, are encountered in clinical practice.
Chronic obstructive lung disease (chronic bronchitis and emphysema) is a risk factor for developing lung cancer, independent of cigarette smoking. In both chronic obstructive pulmonary disease (COPD) and diffuse pulmonary fibrosis, proposed mechanisms of increased cancer risk include decreased clearance of inhaled carcinogens and epithelial metaplasia.
Genetic predisposition plays a role in the development of lung cancer. In general, relatives of subjects with lung cancer have a higher risk of developing lung cancer (about twofold) than the general population. An increased risk of lung cancer has been associated with specific oncogenes, chromosome defects, specific HLA antigens, enzyme defects, and defects in proteins normally produced by tumor suppressor genes.
CELL TYPES OF LUNG CANCER
Lung carcinomas have been classified by the World Health Organization (WHO) based on their light-microscopic appearances (Table 3-2). The large majority of lung cancers are classified by WHO criteria as one of four major histologic types: squamous cell carcinoma, adenocarcinoma, small cell carcinoma, and large cell carcinoma. Numerous subtypes of these four major tumors have also been defined, but most of these are unimportant from a radiologic or clinical standpoint.
These cell types are not absolutely distinct. As many as 50% of lung tumors have mixed appearances, and the most differentiated feature of the carcinoma is used to define its cell type. Many tumors classified as one histologic type (e.g., large cell carcinoma) using light microscopy and the WHO system would be reclassified if electron microscopy were used. Cytologic examination uncommonly allows a specific cell type to be determined; cytologic diagnosis of lung cancer is usually limited to the designation nonsmall cell lung carcinoma (NSCLC) or small cell carcinoma.
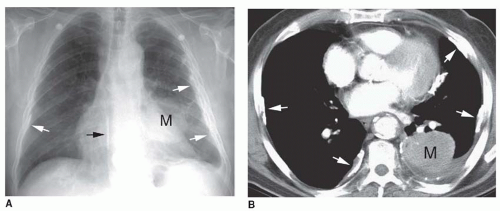
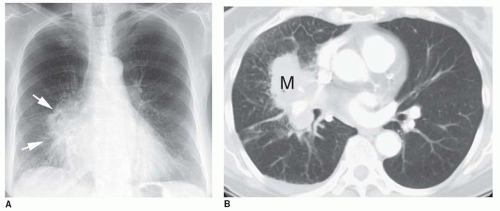
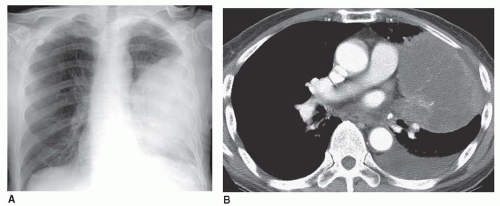
FIG. 3.1. Lung cancer associated with asbestos exposure. A: Chest radiograph shows a large left lung mass (M) representing lung cancer. Bilateral pleural thickening with calcification is also visible (arrows). B: CT shows a left lung mass (M) and bilateral localized calcified pleural plaques (arrows) typical of asbestos exposure.
Preinvasive Lesions
These lesions are dysplastic or localized and include atypical adenomatous hyperplasia (AAH), squamous dysplasia and carcinoma in situ, and diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (described below along with carcinoid tumors).
AAH represents a bronchioloalveolar proliferation that resembles but does not meet the criteria for bronchioloalveolar carcinoma (BAC). Its incidence ranges from 5% to 20%. Most lesions are 5 mm or less in diameter, and lesions are often multiple. AAH is most often found incidentally in pathologic specimens but may mimic lung carcinoma radiographically (particularly on CT), leading to resection. On CT, AAH typically appears as a small nodule of ground-glass opacity.
TAB L E 3.1 Increased Risk of Lung Cancer Associated With Smoking and Asbestos Exposure
Risk Factor
Comparison Group
Relative Risk
Heavy asbestos exposure
No asbestos exposure
5:1
Heavy smoking
Nonsmoker
20:1
Heavy smoking and heavy asbestos exposure
No smoking history and no asbestos exposure
100:1
Squamous Cell Carcinoma
Until recently, squamous cell carcinoma was the most common cell type of lung carcinoma; it currently accounts for about 30% of cases. It is strongly associated with cigarette smoking (Table 3-3).
Squamous cell carcinoma frequently (65%) arises in main, lobar, or segmental bronchi. In this location, tumor growth results in obstruction of the bronchial lumen, infiltration of the bronchial wall, and invasion of the adjacent lung or vessels. This tumor tends to cause symptoms early in its course because of its proximal and endobronchial location and may be detected using sputum cytology before being radiographically visible. Early metastasis is uncommon, and it has a relatively good 5-year survival rate.
TABLE 3.2 Classification of Lung Carcinoma and Important Subtypes From the 1999/2004 WHO Classifications
Preinvasive lesions
Atypical adenomatous hyperplasia
Squamous cell carcinoma
Adenocarcinoma
Bronchioloalveolar carcinoma
Nonmucinous
Mucinous
Adenocarcinoma, mixed subtype
Small cell carcinoma
Large cell carcinoma
Large cell neuroendocrine carcinoma
Adenosquamous carcinoma
Carcinoma with pleomorphic, sarcomatoid, or sarcomatous elements
Carcinoid tumor
Typical carcinoid tumor
Atypical carcinoid tumor
Carcinomas of salivary gland type
Adenoid cystic carcinoma
Mucoepidermoid carcinoma
(Modified from Travis WD. Pathology of lung cancer. Clin Chest Med 2002; 23:65-81.)
TABLE 3.3 Squamous Cell Carcinoma
30% of lung cancer cases
Strongly associated with cigarette smoking
65% arise in main, lobar, or segmental bronchi
Endobronchial mass
Bronchial obstruction
Infiltration of bronchial wall
Local invasion
Hilar mass
Atelectasis and consolidation common
30% present as solitary nodule or mass
Cavitation relatively common
Metastasizes late
Relatively good prognosis
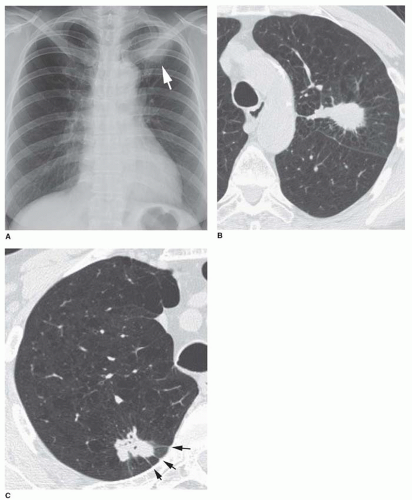
A polypoid endobronchial mass or bronchial obstruction is frequently seen (Fig. 3-2A). Hilar mass is also common due to the central location of the tumor, with local invasion and involvement of hilar lymph nodes (see Fig. 3-2B). Atelectasis (Fig. 3-3), consolidation, mucoid impaction, and bronchiectasis are common radiographic findings, reflecting the presence of bronchial obstruction (see Table 3-3). Only about 30% of squamous cell carcinomas present in the lung periphery as a lung nodule. Central necrosis and cavitation (Fig. 3-4) are more common than with other cell types.
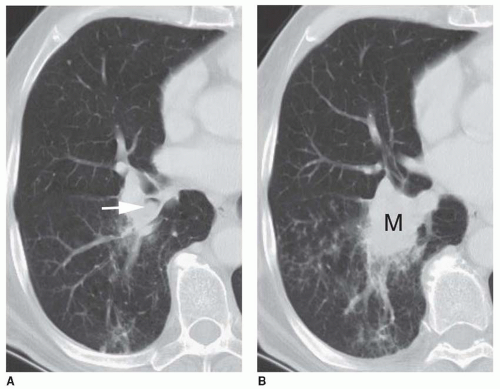
FIG. 3.2. Squamous cell carcinoma with an endobronchial and hilar mass. A: CT shows a polypoid mass (arrow) within the right lower lobe bronchus, typical of squamous cell carcinoma. B: At a slightly lower level, the bronchial lumen appears obstructed and local invasion has resulted in a hilar mass (M).
Adenocarcinoma
Adenocarcinoma is the most common cell type of lung cancer and accounts for 30% to 35% of lung cancer cases (Table 3-4). As with squamous cell cancer, it is related to cigarette smoking, although its association with smoking is relatively weak. Adenocarcinoma is thought to arise from bronchiolar or alveolar epithelium and is characterized by glandular differentiation. Invasion of lung parenchyma is usually present. Early metastasis is more common than with squamous cell carcinoma, particularly to the central nervous system and adrenal glands. Seventy-five percent originate in the lung periphery, presenting as a solitary pulmonary nodule (Fig. 3-5). In a few cases, adenocarcinoma originates within large airways. It is most common in the upper lobes. It is often associated with fibrosis; it may arise in relation to preexisting lung fibrosis (i.e., a scar carcinoma) or may result in a desmoplastic reaction in surrounding lung.
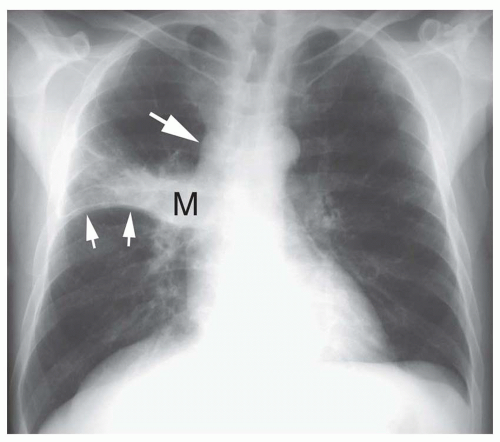
FIG. 3.3 Squamous cell carcinoma with bronchial obstruction and atelectasis. Chest radiograph shows a right hilar mass (M) with upward bowing of the minor fissure (small arrows). This combination results in Golden’s S sign. Mediastinal lymph node enlargement is also present (large arrow).
Adenocarcinomas often appear ill defined on chest radiographs because of their irregular margin (see Fig. 3-5A). On high-resolution CT, adenocarcinoma presenting as a solitary nodule may appear round or lobulated. They frequently have an irregular and spiculated margin because of associated lung fibrosis (see Fig. 3-5B). When occurring in a subpleural location, this may result in thin linear extensions to the pleural surface (i.e., a pleural tail; see Fig. 3-5C). Air bronchograms may be visible within the nodule using CT; although central necrosis is common, cavitation visible on radiographs or CT is uncommon. When adenocarcinoma arises from the wall of a central bronchus, it is radiographically indistinguishable from squamous cell carcinoma.
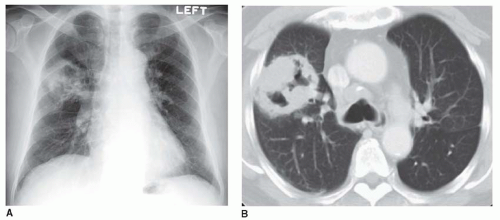
FIG. 3.4. Squamous cell carcinoma with a cavitary lung mass. A: On a chest radiograph, a large, thick-walled cavitary mass is visible in the right upper lobe. B: CT shows the cavity to have a thick and nodular wall. This is typical of cavitary carcinoma. This would be considered a T2 carcinoma.
TABLE 3.4 Adenocarcinoma
30%-35% of lung cancer cases (most common cell type)
Weak association with smoking
Early metastases common
75% present as peripheral lung nodule
Common in the upper lobes
Associated with lung fibrosis
Often appear spiculated
Bronchioloalveolar Carcinoma
BAC is a well-differentiated subtype of adenocarcinoma that also tends to occur in the lung periphery (Table 3-5). In the current WHO classification, BAC is defined as unassociated with invasion of pleura, vessels, or lung stroma. Using this restrictive definition, BAC is relatively uncommon, accounting for fewer than 5% of lung malignancies. It has a very good prognosis when localized, with a 5-year survival rate approaching 100%.
BAC spreads as a thin layer of cells, using the alveolar or bronchiolar walls as a framework or scaffold. This pattern of growth is termed lepidic. Other types of adenocarcinoma usually invade and destroy lung parenchyma as they grow, a pattern termed hilic.
Nonmucinous and mucinous subtypes of BAC occur in about equal numbers. These cell types correlate with radiographic appearance.
FIG. 3.5. Typical appearances of adenocarcinoma. A: Chest radiograph in a patient with adenocarcinoma shows an ill-defined nodule in the left lung apex (arrow). Adenocarcinomas often appear ill defined on radiographs because of their irregular and spiculated edge. B: High-resolution CT in a patient with adenocarcinoma in the left upper lobe shows a solitary lung nodule with an irregular and spiculated edge. Spiculation usually results from lung fibrosis associated with the tumor. This tumor would be classified as a T1 carcinoma in the lung cancer staging system. C: High-resolution CT in a patient with adenocarcinoma presenting as a solitary nodule in the posterior right upper lobe. The nodule appears lobulated and spiculated. Extensions to the pleural surface (arrows) are termed pleural tails. They result from fibrosis with a puckering of the visceral pleural surface.
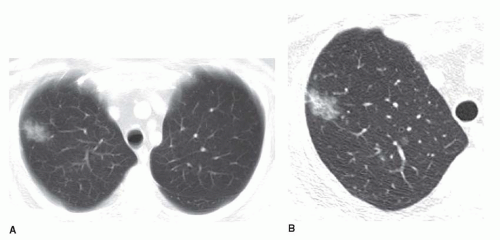
BAC most commonly presents as solitary nodule (60%) and radiographically may be indistinguishable from adenocarcinoma. BAC presenting as a solitary nodule is usually the nonmucinous subtype of BAC. Because of its lepidic growth pattern, radiographs and CT usually show a very ill-defined nodule (Fig. 3-6). On HRCT, localized BAC appears as a ground-glass opacity nodule, sometimes associated with regions of soft tissue attenuation (Fig. 3-7), and often contains air bronchograms or bubbly lucencies. The bubbly lucencies represent cystic air-filled areas within the tumor termed pseudocavitation (see Fig. 3-6B).
TABLE 3.5 Bronchioloalveolar Carcinoma
Subtype of adenocarcinoma
Noninvasive tumor characterized by lepidic growth
60% present as a solitary nodule
Usually nonmucinous cell type
Ill-defined nodule of ground-glass opacity
Air bronchograms and cystic areas (pseudocavitation)
Excellent prognosis
40% appear as diffuse or patchy consolidation and/or nodules
Mucinous cell type
Lung consolidation due to mucus filling alveoli
CT angiogram sign
Poor prognosis
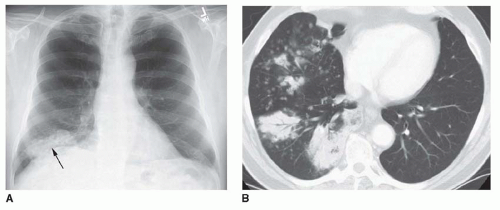
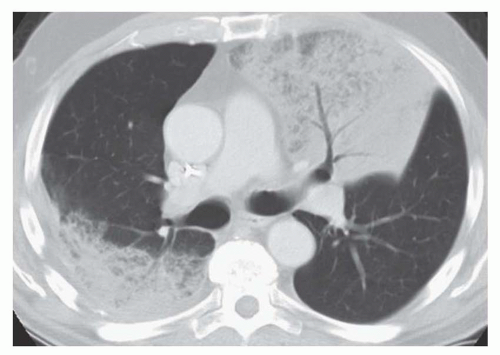
In 40% of cases, BAC presents with diffuse or multifocal lung involvement having the appearance of lung consolidation or multiple ill-defined nodules (Figs. 3-8 and 3-9; see Fig. 3-22). This appearance is typical of the mucinous subtype of BAC. It is unclear whether this pattern results from multicentric origin of the tumor or endobronchial spread. Although lepidic growth is present in such patients, with tumor cells lining alveolar walls, mucin produced by the tumor fills the alveoli, resulting in the radiographic appearance of consolidation. The CT angiogram sign, in which opacified vessels are visible within consolidated lung, is often seen if CT is obtained with contrast infusion (see Chapter 2). Patients with diffuse BAC can present with profuse watery sputum production, termed bronchorrhea, as a result of extensive mucin production. Diffuse BAC has a poor prognosis.
FIG. 3.6. Focal bronchioloalveolar carcinoma (BAC). A: Chest radiograph shows a very ill-defined nodule (arrow) in the left lung. B: CT with 5-mm slice thickness shows an ill-defined, irregular, spiculated nodule, containing both air bronchograms and bubbly lucencies. This appearance is typical of focal BAC.
Adenocarcinoma, mixed subtype
Adenocarcinomas having some characteristics of BAC are common and classified as adenocarcinoma, mixed subtype. They are sometimes referred to as minimally-invasive adenocarcinoma with BAC. These tumors have a prognosis intermediate between invasive adenocarcinoma and BAC. They may resemble either tumor radiographically, appearing as a solid nodule, a nodule of ground-glass opacity, a nodule of mixed attenuation, or as a diffuse or multifocal abnormality.
Small Cell Carcinoma
Small cell carcinoma is the third most common histologic variety of primary lung cancer (15% to 20% of cases) and is made up of small cells, similar in size to lymphocytes, that have scanty cytoplasm (Table 3-6). It is thought to originate from neuroendocrine cells, and electron microscopy shows neurosecretory granules in many cases of small cell carcinoma. Along with carcinoid tumor and atypical carcinoid tumor, small cell carcinoma is considered to be a type of neuroendocrine carcinoma and is described further below. It is a common cause of paraneoplastic syndromes. It is strongly associated with smoking.
FIG. 3.7. Focal bronchioloalveolar carcinoma. A: CT with 5-mm slice thickness shows an ill-de-fined nodule. B: High-resolution CT shows the nodule to be largely of ground-glass opacity. This appearance is typical of carcinoma having lepidic growth.
FIG. 3.8. Diffuse bronchioloalveolar carcinoma. A: Chest radiograph shows consolidation at the right lung base (arrow). B: CT with 5-mm slice thickness shows multiple areas of consolidation, with air bronchograms, and numerous ill-defined nodules. These nodules are typically centrilobular; they represent air-space or acinar nodules and are common with diffuse bronchioloaveolar carcinoma.
FIG. 3.9. Diffuse bronchioloalveolar carcinoma involving both upper lobes, with air-space consolidation and air bronchograms.
TABLE 3.6 Small Cell Carcinoma
15%-20% of lung cancers
Strongly associated with smoking
Neuroendocrine carcinoma
Paraneoplastic syndromes commonly associated
Most occur in main or lobar bronchi
Extensive peribronchial invasion
Large hilar or parahilar mass
Bronchial narrowing
Lymph node enlargement
Metastases at diagnosis in >90%
Prognosis very poor
Small cell carcinoma tends to occur in the main or lobar bronchi and is associated with extensive peribronchial invasion and a large hilar or parahilar mass (Fig. 3-10). Endobronchial tumor masses are less common than with squamous cell carcinoma, but the large tumor mass frequently compresses bronchi (Fig. 3-11). Atelectasis may be associated. This tumor is commonly associated with marked mediastinal lymph node enlargement (Fig. 3-12). It is a common cause of superior vena cava (SVC) syndrome. Presentation as a lung nodule is very uncommon, accounting for less than 5% of cases.
Although the tumor is relatively radiosensitive, its prognosis is very poor because of the frequent presence of distant metastases at the time of diagnosis. Small cell lung cancer is not generally considered amenable to surgical treatment. Over 90% of cases are Stage IV at diagnosis. Reported cases of small cell carcinoma that present as lung nodules or masses, and that have been cured at surgery, may in fact represent misclassified cases of atypical carcinoid.
FIG. 3.10. Small cell carcinoma. A: Chest radiograph show a large right hilar mass (arrows). B: CT shows the large mass (M). Interstitial thickening characterized by interlobular septal thickening in the middle lobe indicates local lymphangitic spread of tumor.
Large Cell Carcinoma
The term large cell carcinoma is used to describe tumors that do not show squamous or adenomatous differentiation or have typical features of small cell carcinoma. Distinction from poorly differentiated squamous cell or adenocarcinoma can be difficult, and in fact many cases classified as large cell carcinoma on the basis of light microscopy are reclassified as other cell types if electron microscopy is used.
Large cell carcinoma accounts for 10% of lung cancers (Table 3-7). It tends to present as a large peripheral mass; more than 60% are larger than 4 cm at presentation (Fig. 3-13). It is similar to adenocarcinoma in its radiologic characteristics (except for its large size), histologic ultrastructure, and survival statistics. As with adenocarcinoma, it tends to metastasize early and has a poor prognosis. It is strongly associated with smoking.
Large cell neuroendocrine carcinoma is an important subtype of large cell carcinoma, differing histologically from other neuroendocrine tumors such as small cell carcinoma and atypical carcinoid tumor. As with small cell carcinoma, it has a very poor prognosis.
Adenosquamous Carcinoma
Adenosquamous carcinoma has mixed histologic characteristics of both adenocarcinoma and squamous cell carcinoma. If light microscopy is used for classification, adenosquamous carcinoma accounts for a few percent of lung cancers at most. If electron microscopy is used, as many as one third of all lung cancers have mixed characteristics. These tumors usually present as masses in the lung periphery and are indistinguishable from adenocarcinoma or large cell carcinoma. Metastases are common. Adenosquamous carcinomas are aggressive and have a poor prognosis.
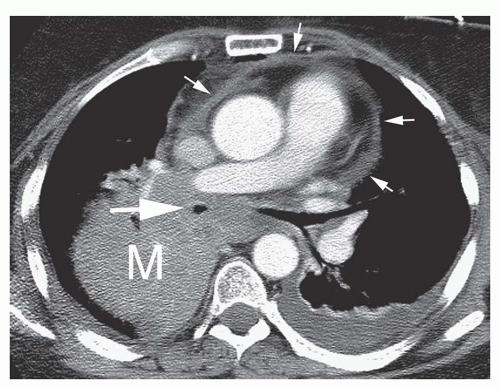
FIG. 3.11. Small cell carcinoma. Contrast-enhanced CT shows a large hilar mass (M). Tumor surrounds and narrows the bronchus intermedius (large arrow) and extends into the subcarinal space. Pericardial thickening (small arrows) is likely due to local invasion. A left pleural effusion is also present.
Carcinoma With Pleomorphic, Sarcomatoid, or Sarcomatous Features
This disparate group of tumors includes those characterized pathologically by a combination of epithelial and mesenchymal tissues (e.g., giant cell carcinoma, carcinosarcoma, pulmonary blastoma). These tumors are rare and may present as polypoid endobronchial masses or large lung masses. Their prognosis is poor.
Carcinoid Tumor
Carcinoid tumor originates from neuroendocrine cells in the bronchial wall. It is classified as typical or atypical carcinoid tumor. Typical carcinoid tumor is a low-grade malignancy and accounts for a few percent of all primary lung malignancies. This tumor most often occurs in the central bronchi, resulting in an endobronchial mass, and is locally invasive. Metastases are relatively uncommon. Atypical carcinoid tumor is a more aggressive variant and has a poorer prognosis. Typical carcinoid tumor, atypical carcinoid tumor, large cell neuroendocrine carcinoma, and small cell carcinoma are considered to be different types of neuroendocrine carcinoma. Carcinoid tumors are discussed in detail below because of their distinct clinical and radiographic appearances.
TABLE 3.7 Large Cell Carcinoma
10% of lung cancers
Strongly associated with smoking
Overlap with other cell types
Usually present as a large peripheral mass (>4 cm)
Metastasizes early
Prognosis poor
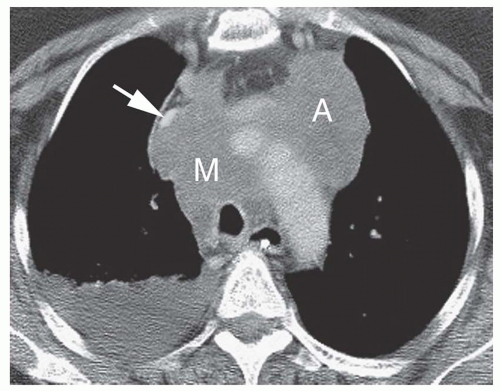
FIG. 3.12. Small cell carcinoma. CT following contrast infusion shows extensive mediastinal lymph node enlargement typical of small cell carcinoma. The superior vena cava (arrow) is displaced anteriorly and markedly narrowed by lymph node mass (M) in the pretracheal space. A large anterior mediastinal lymph node mass (A) is also visible. A right pleural effusion is also present.
Carcinomas of Salivary Gland Type
Salivary gland type carcinomas, also referred to as bronchial gland carcinomas, include adenoid cystic carcinoma (cylindroma) and mucoepidermoid carcinoma. These are similar to salivary gland tumors in their histologic characteristics and arise from glands in the tracheal or bronchial wall. These tumors account for much less than 1% of tracheobronchial malignancies. As with carcinoid tumors, they are locally invasive and uncommonly metastasize, and are discussed in detail below.
RADIOGRAPHIC APPEARANCES OF LUNG CANCER
In most patients with lung cancer, the findings on chest radiographs are sufficiently characteristic to suggest the diagnosis and lead to appropriate clinical and imaging evaluation. Although lung cancer can manifest in a variety of ways, a short list of radiographic abnormalities is commonly seen. These abnormalities reflect the location and manner in which lung cancer arises and the sites to which it most commonly spreads. Such abnormalities include the presence of a lung nodule, evidence of bronchial obstruction with collapse or consolidation of a lobe or lung, a hilar or mediastinal mass, and benign or malignant pleural effusion.
Although the frequency of these findings varies according to the cell type of the tumor (Table 3-8), each of the four major cell types of lung carcinoma (squamous cell carcinoma, adenocarcinoma, small cell carcinoma, large cell carcinoma) can show similar findings. Radiographic findings associated with carcinoid tumor and the bronchial gland carcinomas are discussed later in this chapter because of their somewhat different biological behavior and X-ray appearances.
FIG. 3.13. Large cell carcinoma. A: Chest radiograph shows a large left lung mass. B: On contrast-enhanced CT, a large mass occupies the left lung. A left pleural effusion is also present.
Solitary Pulmonary Nodule or Mass
Approximately one third of lung cancers present radiographically as a solitary pulmonary nodule or lung mass.
A solitary pulmonary nodule (see Figs. 3-5,3-6 and 3-7) is usually defined as being visible as a focal opacity on chest radiographs or CT and is
Relatively well-defined
At least partially surrounded by lung
Roughly spherical
3 cm or less in diameter
Similar lesions larger than 3 cm in diameter are usually referred to using the term mass (see Figs. 3-1, 3-4, and 3-13). This measurement is also used to distinguish a T1 carcinoma (3 cm or less in diameter) from a T2 carcinoma (larger than 3 cm).
TABLE 3.8 Plain Radiologic Findings in Lung Cancer by Cell Typea
Finding
Squamous (%)
Adencarcinoma (%)
Small Cell (%)
Large Cell (%)
Peripheral nodule or mass
30
75
5
65
Atelectasis
40
10
20
15
Consolidation
20
15
20
25
Hilar enlargement
40
20
80
30
Mediastinal mass
<5
<5
15
10
Pleural effusions
5
5
5
5
No abnormalities
5
<5
0
0
Multiple abnormalities
35
30
65
45
aBoldface findings are those most helpful in differentiating cell types. Percentages are approximate.
Among lung cancers presenting as a solitary nodule or mass, the most common cell types are adenocarcinoma (40% of cases), squamous cell carcinoma (20%), large cell carcinoma (15%), and BAC (10%). Since BAC is considered to be a subtype of adenocarcinoma, the adenocarcinomas account for half of the cases (see Figs. 3-5,3-6 and 3-7). Large cell carcinoma typically results in a mass (see Fig. 3-13) that at diagnosis is larger than that seen with other cell types, averaging nearly twice the diameter of adenocarcinoma or BAC. Small cell carcinoma uncommonly results in a solitary nodule.
Lung cancers presenting as a solitary pulmonary nodule may have specific radiographic appearances that suggest the diagnosis (Table 3-9); if a combination of radiologic, clinical, and laboratory information is used, malignant pulmonary nodules can be diagnosed in over 90% of patients. The radiographic assessment of a solitary pulmonary nodule is a common and important problem; this topic is discussed in greater detail in Chapter 9. The differential diagnosis of a solitary nodule is reviewed in Table 9-1 in Chapter 9.
TABLE 3.9 Typical Radiographic Characteristics of Lung Cancer Presenting as a Solitary Pulmonary Nodule
Diameter >2 cm
Most common in the upper lobes
Ill-defined, irregular, or spiculated margin
Lobulated or irregular in shape
Containing air bronchograms or bubbly lucencies (pseudocavitation)
Cavitation with a thick (>15 mm) and nodular wall
Cavitation without an air-fluid level
Satellite nodules absent
Calcification absent or not typical of a benign pattern
Enhancement of ≥15 HU following contrast infusion
Doubling time of 30-200 days (although BAC may be very slow growing, i.e., doubling time >1,000 days)
Superior Sulcus (Pancoast) Tumor
Tumors arising at or near the lung apex are termed superior sulcus carcinoma, thoracic inlet carcinoma, or simply apical carcinoma. The term Pancoast tumor is best reserved for patients with some (although not necessarily all) manifestations of the Pancoast syndrome. Approximately 5% of lung cancers occur in the superior sulcus; any cell type may be responsible.
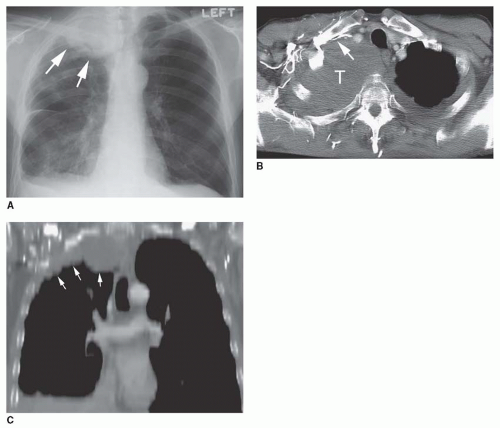
FIG. 3.14. Superior sulcus tumor. A: Chest radiograph shows a mass (arrows) at the right lung apex. B: CT following contrast injection via the right arm shows the tumor (T) occupying the lung apex. Obstruction of the right subclavian vein (arrow) is associated with numerous venous collaterals in the chest wall. C: Coronal CT reformation shows the apical mass (arrows) extending along the chest wall.
Superior sulcus tumors are commonly associated with symptoms because of their propensity to invade structures in the thoracic inlet, including the brachial plexus, cervicothoracic sympathetic ganglia, subclavian artery and vein (Fig. 3-14), and vertebral column. Pancoast syndrome results from involvement of the brachial plexus and sympathetic ganglia and consists of the combination of
Pain in the shoulder
Radicular pain along the distribution of the eighth cervical and first and second thoracic nerves, sometimes associated with wasting of the small muscles of the hand
Horner’s syndrome, consisting of ptosis, miosis, and hemifacial anhidrosis
Classic Pancoast syndrome is uncommon. Most superior sulcus tumors present with shoulder or scapular pain that radiates down the arm and may be associated with ulnar neuropathy. Horner’s syndrome is present in only about 25% of patients; atrophy or weakness of the hand muscles is uncommon. Rib or vertebral body invasion is common in patients with superior sulcus tumors.
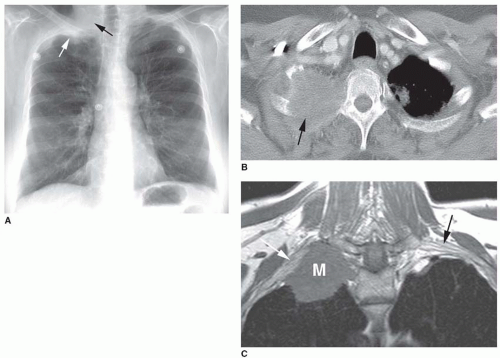
FIG. 3.15. Superior sulcus tumor appearing as an apical cap with bone destruction and invasion of the brachial plexus. A: A right apical Pancoast tumor (white arrow) mimics pleural thickening. The underlying rib is partially destroyed (black arrow). B: CT shows a mass occupying the right apex, with focal rib destruction (arrow). C: T1-weighted MRI shows a mass in the right apex, with invasion of the brachial plexus (white arrow). The normal left brachial plexus is identified for comparison (black arrow).
Radiographic findings include an apical mass (60%; see Fig. 3-14), unilateral or asymmetrical apical pleural thickening (“apical cap,” 40%; Fig. 3-15A), and bone destruction (25%). Asymmetry in the thickness of an apical cap exceeding 5 mm is considered suggestive. The presence of an apical cap may reflect diseases other than carcinoma (Table 3-10).
TABLE 3.10 Differential Diagnosis: Apical Cap/Apical Mass
Normal apical cap: Unilateral or bilateral apical caps, usually <5 mm in thickness, are each seen in 10% of normals on chest radiographs. These represent apical lung scars unassociated with tuberculosis, although their etiology is unclear.
Extrapleural fat: Extrapleural fat deposition can result in smooth, symmetrical apical caps. This can be seen in normals, obese patients, and patients with Cushing’s syndrome or those receiving steroids.
Inflammatory disease (tuberculosis): Apical caps associated with inflammatory disease (particularly TB) are rarely the only abnormality visible. Associated upper lobe fibrosis, volume loss, lung destruction, or other evidence of inflammatory disease is usually present. The cap is often quite irregular in appearance because of adjacent lung abnormalities and in one study ranged from 5 to 27 mm in thickness (mean 16.5 mm). In patients with TB, thickened extrapleural fat accounts for most of the apical cap, variably associated with thickening of the pleura and atelectatic lung.
Superior sulcus carcinoma
Neural tumor or other posterior mediastinal mass: These are typically localized masses.
Mesothelioma: Diffuse pleural thickening is often seen.
Mediastinal hemorrhage: Mediastinal blood can dissect laterally in the extrapleural space over the lung apex, resulting in a smooth apical cap. This can be seen with traumatic aortic rupture and is more common on the left.
Radiation fibrosis: Radiation therapy can result in apical lung fibrosis mimicking an apical cap. This is most common following head and neck or supraclavicular node radiation.
Peripheral upper lobe collapse: Peripheral upper lobe collapse is said to be present when the peripheral part of a collapsed upper lobe is pancaked against the apical pleural surface (see Fig. 2-34). It has been reported in a variety of conditions, including inflammatory diseases and bronchial obstruction.
Superior sulcus carcinomas, even if invasive, can be treated using a combination of radiation and en bloc resection of the tumor and adjacent chest wall; 5-year survival rates as high as 30% to 35% have been reported using this approach. Contraindications to this combined therapy generally include (1) tumor involvement of the great vessels above the lung apex, principally the subclavian artery or vein; (2) extensive brachial plexus invasion; (3) extensive vertebral body or spinal canal invasion; (4) clinical evidence of recurrent laryngeal nerve or phrenic nerve involvement; (5) involvement of the mediastinum, including the trachea or esophagus; and (6) distant metastases. Some patients may have restaging of an extensive tumor following chemotherapy to determine whether resection is possible.
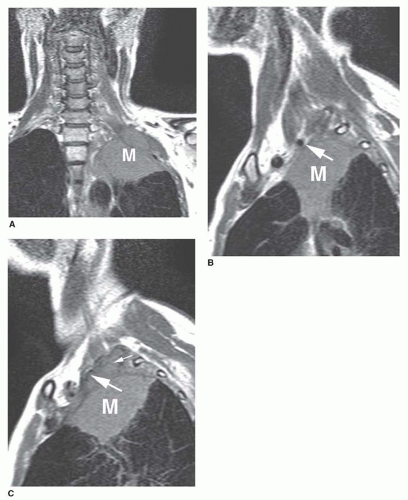
FIG. 3.16. MRI of superior sulcus tumor. A: Coronal T1-weighted image shows an apical mass (M) with extension into the chest wall. B: Sagittal T1-weighted MRI shows the mass (M) occupying the lung apex. The left subclavian artery (arrow) appears normal. C: More laterally, the mass (M) invades the chest wall (small arrow) with narrowing of the left subclavian artery (large arrow).
MRI in the sagittal or coronal planes is advantageous in imaging apical tumors. It is more accurate than CT in diagnosing apical chest wall invasion and its extent. MRI is often obtained preoperatively in patients with superior sulcus carcinoma to define the relationship of the tumor to great vessels and the brachial plexus (Figs. 3-15 and 3-16). The radiographic assessment of chest wall invasion and superior sulcus tumor is discussed in detail in the section on lung cancer staging below.
TABLE 3.11 Differential Diagnosis of Bronchial Narrowing or Obstruction
Airway abnormalities are common in lung cancer. The segmental bronchi are most often involved by the primary tumor, followed in frequency by the lobar bronchi and the main bronchi. The trachea is rarely involved as the site of origin.
Radiographs or CT can show evidence of bronchial narrowing or obstruction, or abnormalities secondary to bronchial obstruction, such as mucous plugging, air trapping, atelectasis, or obstructive pneumonia. Although lung cancer is a common cause of bronchial obstruction, the differential diagnosis is long and should be kept in mind (Table 3-11).
Bronchial Abnormalities
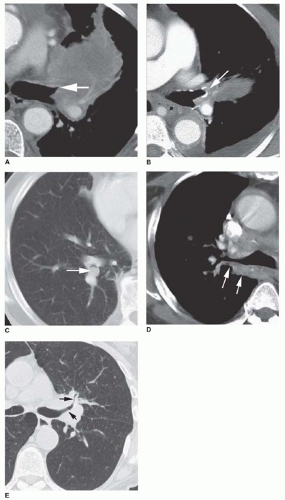
Bronchial abnormalities sometimes can be recognized on chest radiographs in patients with lung cancer, but CT is much more sensitive. Abnormalities include
Narrowing or tapering of the bronchial lumen, a finding that reflects the tendency of lung carcinomas to infiltrate along the bronchial wall (Fig. 3-17A); a tapered narrowing, or “rat-tail,” appearance of the bronchial lumen is highly suggestive of carcinoma.
Sharp cutoff of the bronchial lumen (see Fig. 3-17B)
An endobronchial mass, sessile, irregular, or polypoid in appearance (see Figs. 3-2A and 3-17C)
Bronchial wall thickening, most easily seen involving the posterior wall of the right upper lobe bronchus or bronchus intermedius (see Figs. 3-17D and 3-24B)
Smooth luminal narrowing caused by bronchial wall infiltration or bronchial compression by an extrinsic mass (see Figs. 3-17E and 3-24B).
CT is commonly used to identify bronchial abnormalities in patients with lung cancer, in conjunction with bronchoscopy. CT can serve to identify the bronchi involved by the mass, thus guiding bronchoscopy, and can better assess the presence and degree of tumor extension outside the bronchus.
Generally speaking, the CT findings of an endobronchial lesion, an abrupt bronchial occlusion, or bronchial wall irregularities correlate closely with what is seen at bronchoscopy, but the appearances of smooth luminal narrowing or tapered bronchial occlusion can be seen with either endobronchial disease or extrinsic mass.
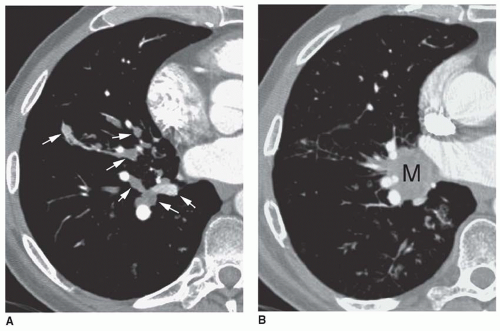
Mucous Plugging
Rarely, an obstructing or partially obstructing tumor causes retention of mucus distal to the obstruction, while the lobe remains aerated because of collateral ventilation. This can result in a mucous plug or plugs visible on radiographs or CT (Fig. 3-18). It can be recognized on plain film or CT by its typical branching, “finger-in-a-glove,” or clusteredgrape appearance. On CT, mucous plugs appear low in attenuation.
More common causes of mucous plugging include asthma, allergic bronchopulmonary aspergillosis, and cystic fibrosis. In patients with these diseases, however, mucous plugs are usually multiple and bilateral. In a patient with focal mucous plugging, bronchoscopy is advisable to rule out an obstructing lesion. In addition to lung cancer, focal mucous plugging can result from benign tumors, strictures, or congenital bronchial atresia.
Air Trapping
An obstructing or partially obstructing carcinoma rarely causes air trapping within the lung distal to the tumor. If a lobar bronchus is involved, the volume of the lobe may be increased. If the lesion involves a main bronchus, the distal lung is of normal or slightly decreased volume on inspiration, but on expiration air trapping will be recognized. In some patients, bronchial obstruction and air trapping can be detected because of hypovascularity of the involved lobe or lung; poorly ventilated lung tends to be poorly perfused.
Tracheal Carcinoma
Less than 1% of lung carcinomas arise in the trachea. Squamous cell carcinoma and carcinomas of mucous gland origin (adenoid cystic carcinoma) occur in nearly equal numbers. Squamous cell carcinomas arise most commonly in the distal trachea (Fig. 3-19), near the carina, and may cause obstruction of a main bronchus; adenoid cystic carcinoma is most common in the proximal trachea and often arises from the posterior or lateral tracheal wall.
FIG. 3.17. Bronchial abnormalities in lung cancer. A: The left upper lobe bronchus is obstructed and shows a tapered narrowing or rat-tail appearance (arrow). Left upper lobe atelectasis is also present. B: Left upper lobe carcinoma (arrow) associated with sharp cutoff of the bronchial lumen. C: A polypoid carcinoma (arrow) is visible in the right lower lobe bronchus, outlined by a crescent of air. D: Thickening of the posterior wall of the right upper lobe bronchus (arrows) associated with right hilar carcinoma. This usually indicates bronchial infiltration. E: Narrowing of the left upper lobe and anterior segment bronchi (arrows) by a left hilar carcinoma. This may be caused by tumor infiltrating the bronchial wall or compression by an extrinsic mass.
FIG. 3.18. Mucous plugs in a patient with carcinoma and bronchial obstruction. A: Mucous plugs (arrows) fill lower lobe bronchi. Note that the mucus-filled bronchi lie adjacent to opacified pulmonary arteries. The distal lung remains aerated. B: At a higher level, a hilar mass (M) is associated with obstruction of the right lower lobe bronchus.
Radiographic studies may be important in suggesting the diagnosis, because symptoms are often late and nonspecific. Radiographic findings are similar to those seen with tumors affecting the bronchi. However, findings of obstructive pneumonitia or air trapping are not seen unless there is secondary involvement of a main bronchus. Focal tracheal narrowing associated with thickening of the right paratracheal stripe, a focal endotracheal lesion, or mediastinal mass are most commonly seen on radiographs (Fig. 3-20A). Invasion of the mediastinum may occur. If the mass extends posteriorly, esophageal obstruction can result (see Fig. 3-20B). If a tracheal lesion is suspected on plain radiographs, evaluation using CT and bronchoscopy is appropriate. Surgery can be curative if the diagnosis is made prior to mediastinal invasion. Tracheal tumors are also discussed in Chapter 22.
Only gold members can continue reading. Log In or Register to continue