Abstract
FDG PET/CT has become an important modality in the evaluation of lymph nodes in oncology patients, including the central role FDG PET/CT plays in managing patients with lymphoma and the ability for FDG PET to detect nodal metastases in subcentimeter nodes which may be overlooked on CT or magnetic resonance. However, it is important to realize that there are multiple benign causes for FDG avidity in nodes, which must be distinguished from malignancy. The spatial distribution of the nodes, the corresponding CT findings, and the clinical history will help distinguish benign FDG-avid nodes from malignancy.
Keywords
FDG, PET/CT, lymph nodes, lymphoma, Lugano classification, nodal metastases, sarcoid
18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) has become an important modality in the evaluation of lymph nodes in oncology patients, including the central role FDG PET/CT plays in managing patients with lymphoma and the ability for FDG PET to detect nodal metastases in subcentimeter nodes which may be overlooked on CT or magnetic resonance (MR). However, it is important to realize that there are multiple benign causes for FDG avidity in nodes, which must be distinguished from malignancy. The spatial distribution of the nodes, the corresponding CT findings, and the clinical history will help to distinguish benign FDG-avid nodes from malignancy.
Lymphoma
FDG PET/CT has become the primary imaging modality for staging and treatment response in patients with FDG-avid lymphomas. The vast majority of lymphomas are FDG avid, including the most common lymphomas, Hodgkin lymphoma (HL), diffuse large B-cell lymphoma(DLBCL), and follicular lymphoma. Some lymphomas have variable FDG avidity, including chronic lymphocytic leukemia/small lymphocytic lymphoma, lymphoplasmacytic lymphoma, and marginal zone lymphoma. FDG PET/CT would be useful in these lymphomas only if the tumor in an individual patient was proven to be FDG avid. In non–FDG avid lymphomas, contrast-enhanced CT is the standard imaging modality.
The most recent recommendations for the use of FDG PET/CT are referred to as the Lugano Classification. These guidelines were produced following an International Conference on Malignant Lymphoma held in Lugano, Switzerland. These consensus guidelines state that FDG PET/CT should be recommended for the initial staging of FDG-avid nodal lymphomas. A biopsy is needed to confirm that FDG-avid nodes represent lymphoma. The intensity of FDG avidity (the standardized uptake value max [SUVmax] of the node) cannot be used to diagnosis lymphoma in lieu of a biopsy. However, after lymphoma has been diagnosed by biopsy, the SUVmax can be used to help distinguish low-grade from high-grade lymphoma. As a rule of thumb, a pretreatment SUV of greater than 20 indicates high-grade lymphoma (see Chapter 13 , Fig. 13.2 ), whereas SUV less than 10 is typically a low-grade lymphoma (see Chapter 13 , Fig. 13.3 ). Values between 10 and 20 are usually high-grade lymphomas, but there is some overlap. This is valuable for patients for whom malignant transformation from a low-grade lymphoma to a more aggressive high-grade lymphoma is suspected. FDG PET/CT can identify if there are any lesions of high FDG avidity, suspicious for transformation, that have developed and can direct biopsy to an accessible highly FDG-avid lesion.
Focal FDG avidity within the bone or bone marrow is highly sensitive for osseous lymphoma in FDG-avid lymphomas. Conversely, homogenous elevation of FDG avidity in the bone marrow is usually bone marrow repopulation (see Chapter 3 , Fig. 3.11 ). Evaluation of the osseous structures on FDG PET/CT is so sensitive for bone marrow involvement that routine bone marrow biopsy is no longer indicated for most patients with HL and DLBCL. Splenic, liver, and other organ involvement is also best evaluated by FDG PET/CT, despite physiologic activity in some organs. Only the central nervous system is described to be best evaluated by another imaging modality, MR, rather than FDG PET/CT.
Following treatment, FDG PET/CT is more accurate in determining treatment response than is CT for FDG-avid lymphomas. A five-point scale (5PS) is described in the Lugano Classification, which provides high interobserver assessment of lymphoma treatment response. The 5PS scores the greatest residual FDG avidity at a site of initial disease as follows:
- 1.
No FDG uptake
- 2.
Uptake less than or equal to mediastinal background
- 3.
Uptake greater than mediastinal background but less than or equal to liver background
- 4.
Uptake “moderately” higher than liver
- 5.
Uptake “markedly” higher than liver or new lesions
For most clinical situations, a 5PS of 1, 2, or 3 represents a complete metabolic response, without evidence of residual active lymphoma ( Figs. 21.1 and 21.2 ). Even if there are residual masses, a complete metabolic response is considered a complete remission of lymphoma. A 5PS of 4 or 5 represents residual active lymphoma ( Figs. 21.3 to 21.5 ). The terms “moderately” and “markedly” higher than liver are not defined, but many people interpret “markedly” to be more than twice the liver background. In general, if the SUV is decreasing, the score of 4 or 5 represents a partial metabolic response. If the SUV is without significant change, then the score of 4 or 5 represents stable metabolic disease. And if the SUV is increasing, or there are new FDG-avid lesions representing lymphoma, the score should be a 5.
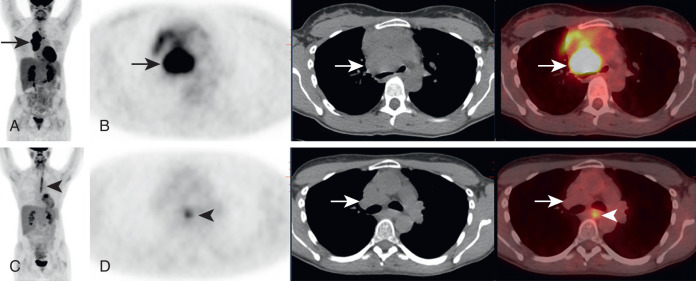
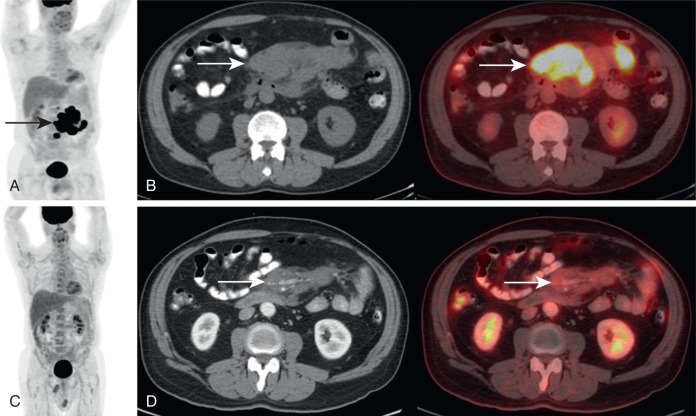
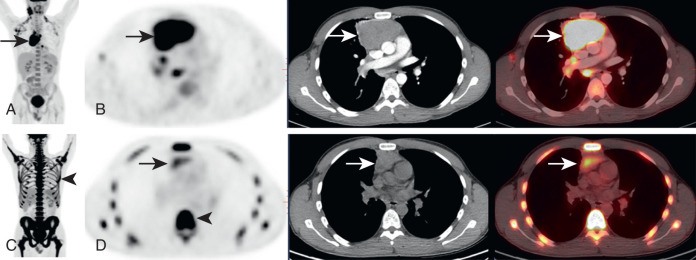
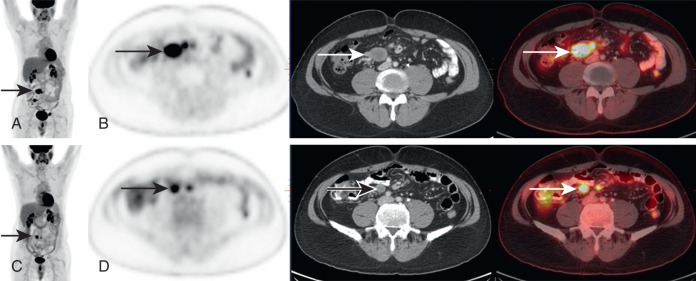
There is a distinction between an “interim” scan (one that is performed in the middle of planned therapy) and an “end of treatment” scan (one that is performed after the course of therapy is finished). For an interim PET/CT, a 5PS score of 1, 2, or 3 is a highly desired result. A 5PS of 4 or 5 with decreasing SUV suggests the disease is responding, and treatment is continued. A 5PS of 5 with increasing SUV suggests treatment failure and may prompt a treatment change. For an end of treatment PET/CT, a 5PS of 1, 2, or 3 is again the desired result. But a 5PS of 4 or 5 represents a treatment failure, even if FDG avidity has decreased. That may prompt a biopsy to prove residual active malignancy and necessitate additional treatment. In most cases, for an end of treatment scan, the critical distinction is distinguishing between a 5PS score of 1 to 3 (treated disease) and 4 to 5 (residual active lymphoma), based on whether the treated lymphoma demonstrates FDG avidity less than or greater than liver background.
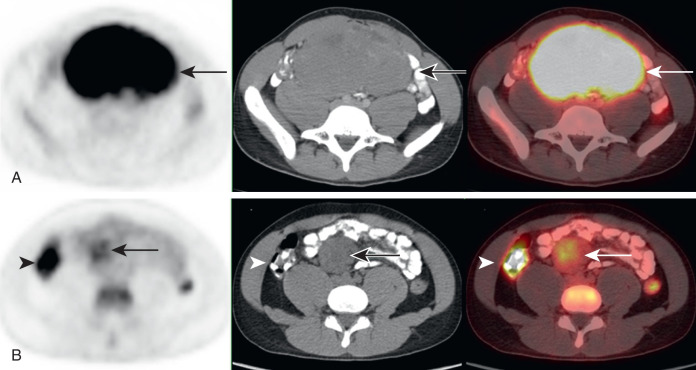
New sites of FDG avidity on posttherapy scans should be scrutinized to determine if the FDG avidity corresponds to a new site of lymphoma or represents a benign cause of FDG avidity. If the new FDG avidity is believed to be benign, the scan can be scored as if the benign FDG avidity does not exist (see Figs. 21.1, 21.3, and 21.4 ). Chemotherapy and radiation may also induce treatment-related inflammation, which may be FDG avid. To minimize posttreatment inflammation, it is recommended to wait at least 3 months following radiotherapy and 3 weeks following chemotherapy before obtaining a FDG PET/CT. Some 5PS scores of 4 may actually represent posttreatment inflammation, rather than residual active malignancy, but this is difficult to distinguish without follow-up imaging or tissue sampling.
After a lymphoma patient has a complete remission, there is no evidence that routine surveillance FDG PET/CT scans provide value. If there are specific signs or symptoms of recurrence, FDG PET/CT is a value method to evaluate for recurrent lymphoma.
With the success of FDG PET/CT in patients with lymphoma, there is debate whether the CT needs to be performed with intravenous (IV) contrast. IV contrast may identify additional findings but rarely changes patient management. IV contrast is valuable for radiotherapy planning and when measurement of nodal size is needed as part of a clinical trial.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


